Pain: from physiopathology to bio-psycho-social model
Review
Pathos 2024; 31. 2. Online 2024, Oct 30
_________________________________________________________________________________
Francesco Amato,1 Erminia Gilda Morrone 2
1 Head of Pain Therapy Unit and CP, Cosenza, Italy
Regional Hub Center
2 Biologist, Pain Therapy Center Ass, Cosenza, Italy
Regional Hub Center
_________________________________________________________________________________
Summary
Pain management is one of the most challenging aspects of medicine and a fundamental part of disease management. Pain sensation is the result of a complex interactions between peripheral nerves and the central nervous system. However, pharmacological and non-pharmacological strategies sometimes prove to be efficacy. Our observations suggest that emotions, nostalgia, cultural and ethnic differences, and relationships with others may serve as potential mechanisms of analgesia, influencing the efficacy of pharmacological treatment.
Riassunto
Il trattamento del dolore rappresenta uno degli aspetti più impegnativi della medicina, e costituisce un aspetto fondamentale della gestione della malattia. La sensazione “dolore” è il risultato di una complessa interazione tra nervi periferici e sistema nervoso centrale; tuttavia, le strategie farmacologiche e non farmacologiche si rivelano talvolta non esaustive. Abbiamo osservato come le emozioni, la nostalgia, le differenze culturali ed etniche, il rapporto con gli altri suggeriscano un possibile meccanismo di analgesia nel modulare l'efficacia del trattamento farmacologico.
Key words
Pain, TRPV1 receptors, bio-psycho-social model, relationship, modulation.
Parole chiave
Dolore, recettori TRPV1, modello bio-psico-sociale, relazioni, modulazione
Introduction
Pain management represents one of the most challenging aspects of medicine and a fundamental part of disease management. The sensation of pain is the result of a complex interaction between peripheral nerves and the central nervous system. However, pharmacological and non-pharmacological strategies are not always effective. Our observations suggest that emotions, nostalgia, cultural and ethnic differences, and relationships with others may serve as potential mechanisms of analgesia, influencing the efficacy of pharmacological treatment.
Pathogenesis
There are a large number of pathologies characterized by pain, but the pathogenetic mechanisms underlying them can be traced to a few basic cases:
- nociceptive pain (generally physiological, high threshold);
- acute inflammatory nociceptive pain;
- chronic pain (low threshold);
- neuropathic pain (including localized neuropathic pain).
It has been demonstrated that physiological, high-threshold nociceptive pain, which is caused by thermal, chemical and mechanical stimuli of high intensity, has a protective effect. This is also the response that occurs in the event of an injury, for example, of a traumatic nature.
While skin nociceptors are particularly sensitive to thermal stimuli, nociceptors in deep somatic tissues, such as joints and muscles, are especially sensitive to mechanical stimuli.
A noxious thermal stimulus is detected by TRPV1 receptors (40 to 43 degrees Celsius)3-5 The application of heat results in a conformational change within the non-selective cation (Ca²⁺) channel of TRPV1, which causes a local depolarization. This is then propagated by the opening of voltage-dependent sodium channels, generating an action potential that travels to the higher centers.6
Inflammatory pain can affect various structures and is characterized by the activation of peripheral nociceptors.
Acute pain is still within a physiological range, inflammation is the body's normal response to tissue damage caused by the presence of pathogens such as viruses, bacteria, fungi and parasites.
Physical trauma, burns, radiation and frostbite are other possible causes of inflammation, such as corrosive chemicals such as acids, alkalis and oxidizing agents.
Symptoms of acute inflammation include swelling, redness, fever and/or pain. Pain is caused in part by tissue distortion due to swelling, but also by certain chemical mediators of inflammation such as bradykinin, serotonin and prostaglandins.
Neutrophils are the first and predominant cells in the acute phase of inflammation. Neutrophils contain granules rich in lysozyme, matrix metalloproteinases and myeloperoxidases, which are released on the foreign or self-antigen and cause its destruction. Neutrophils also destroy the antigen by phagocytosis, release of reactive oxygen species and cytokines such as IL-1, IL-6 and TNF-α.
Lymphocytes, T-lymphocytes and B-lymphocytes constitute the subsequent line of defence and play a pivotal role in mediating inflammation through a multitude of intricate mechanisms, including cytokine secretion, lymphocyte costimulation and the production of antibodies and immune complexes.7
In this context, pain is associated with a reduction in the nociceptive threshold, resulting from the influence of inflammatory mediators, particularly prostaglandins. In the event of persistent pain, cytokines become involved.
Proinflammatory agents, via their receptors, induce biochemical alterations at the nociceptive terminal. To illustrate, the TRPV1 receptors, which normally open at 43°C, undergo phosphorylation due to prostaglandin- and cytokine-activated kinases, leading to activation at 37°C. This body temperature is sufficient to elicit pain. As the threshold is reduced, innocuous stimuli at the site of inflammation cause pain, a phenomenon known as allodynia.
Cronicization
These impulses reach the central synapse, which in turn is modified by the opening of glutamate-sensitive MNDA receptors. Calcium is the second messenger that activates kinases that go into the nucleus of the nerve cell and modify its gene expression. In short, as we move towards chronicity, there is a profound change in the pain pathway: inadequate resolution of inflammation or inadequate control of inflammation can lead to a persistent inflammatory state.
The aim of anti-inflammatory therapies is therefore primarily to reduce peripheral sensitization by blocking the synthesis of prostaglandins and cytokines.
Neuropathic pain
Neuropathic pain (NP) is a direct consequence of an injury or pathology affecting the somatosensory system, whether peripherally or centrally.
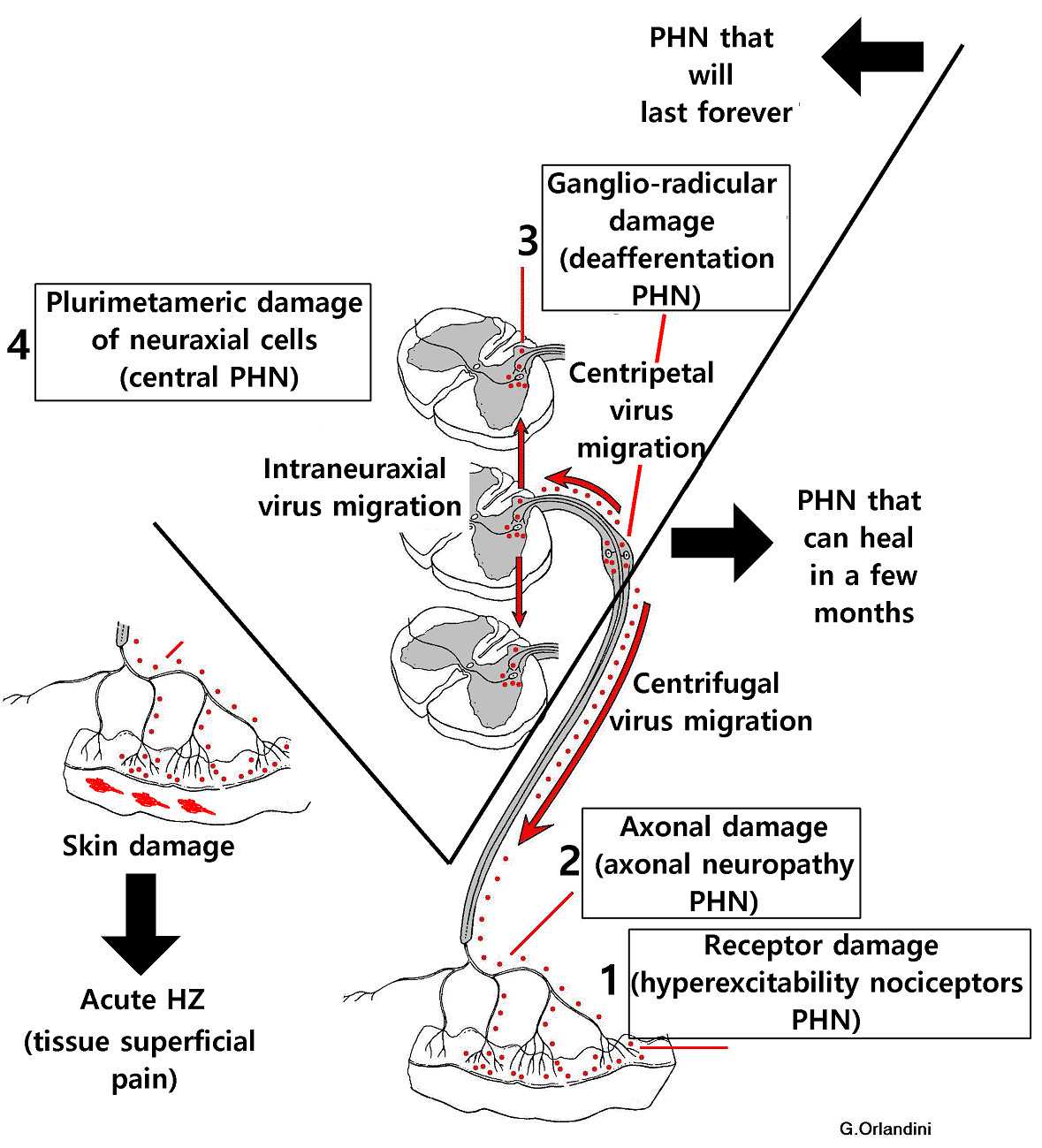
It may result from specific endocrine dysfunctions (painful diabetic peripheral neuropathy), viral infections (post-herpetic neuralgia), trauma (spinal cord injury) or as a consequence of various treatments (chemotherapy-induced peripheral neuropathy). Additionally, neuropathic pain has been linked to various other conditions, including cancer and neurological disorders such as multiple sclerosis, stroke, and centralized pain syndromes.
It is often the case that neuropathic pain has a compressive origin or is related to the injury of a nerve fibre.
In the vicinity of the lesion site of peripheral afferent nerves, which represent the primary site of neuropathic pain, the presence of immune cells has been observed. This is followed by a prolonged release of cytokines and multiple alterations in gene expression.
At the site of the lesion, there is also a functional reorganization of the fiber, with the expression of sodium channels of a different type (embryonic) and a decrease in potassium channels that normally confer electrical stability to the neuron. This results in the formation of an ectopic site (pain does not originate from the periphery) with a high discharge frequency, either spontaneous or evoked, depending on the pathology.
Inhibitory drugs that reduce the discharge of voltage-dependent sodium channels are a potential avenue for treatment.
The spinal cord represents the initial integrating station for nociceptive stimuli originating from the periphery, and is implicated in the pathogenesis of both inflammatory and peripheral neuropathic pain.8
Following the application of chronic stimuli, the spinal cord also exhibits a reduction in its nociceptive threshold, a phenomenon known as spinal sensitization. This is attributed to biochemical changes, predominantly occurring in the spinal neuron.
The increased activity of the N-methyl-D-aspartate (NMDA) receptor in the spinal cord plays a pivotal role in the induction of central sensitisation, which is a crucial process in the development and maintenance of pain hypersensitivity.9
Under physiological conditions, NMDA receptors are blocked by magnesium.
However, under pathological conditions, the magnesium blockade of NMDA receptors is removed and NMDA receptor activation increases by several mechanisms, including phosphorylation of the same.10
Recent studies have also highlighted an interaction between NMDA receptors and TRPV1 receptors at the level of the spinal cord in guinea pigs, which appears to be involved in the transmission of inflammatory and neuropathic pain.
TRPV1 is present at both presynaptic and postsynaptic spinal levels and is associated with the mechanisms of neuropathic pain exacerbation.11 Furthermore, persistent glutamate-mediated hyperexcitability also contributes to the impairment of GABAergic inhibitory tone in the dorsal horn of the spinal cord (DH).
Additionally, the early increase in oxygen free radicals due to oxidative stress has been observed to cause a reduction in GABAergic neurotransmission. This occurs through the modulation of GABAA chloride channels, which in turn attenuates inhibitory synaptic transmission in the superficial dorsal horn.12
Furthermore, over-regulation of P2X4 receptors (at the level of the glia) has been observed, resulting in the release of brain-derived neurotrophic factors (BDNF). This in turn causes changes in the membrane anion gradient. This also contributes to the failure of the excitatory signal normally induced by GABA to be reduced.13
The role of the rostral ventromedial medulla (RVM)
The rostral ventromedial medulla (RVM) plays a pivotal role in supraspinal analgesia, particularly in the context of opioid-induced analgesia, by acting as a key mediator at higher centres. In this region of the brainstem, two distinct types of physiologically definable neuronal cell structures have been identified that are responsive to opioid action. The "off" cells, which are activated by morphine and inhibit the transmission of nociceptive signals, and the "on" cells, which play a pronociceptive role when their activity is depressed, are two distinct types of neuronal cell structures in the rostral ventromedial medulla (RVM).14
Furthermore, opioids interact with additional regions of the brain, including the periaqueductal grey (PAG) and the locus coeruleus, which collectively influence the final passage of nociceptive information to the dorsal horn of the spinal cord.15
The PAG receives signals from the frontal cortex, amygdala and hypothalamus and projects inputs to the RVM and the inferior brainstem, thereby influencing pain perception (Zhang & Lee, 2018). In summary, the PAG integrates these signals and transmits them to the RVM, which can promote and/or inhibit pain according to specific activation pathways (Kwon et al, 2014).
The role of the higher centres
There are several key players in the processing of pain:
the anterior cingulate cortex (ACC) which plays a key role in the processing of pain and related emotions 16,17 and connects extensively with the brainstem and midbrain, including the rostral ventromedial medulla RVM.15
In contrast, the amygdala plays a pivotal role in affective pain, which is a subcortical region that shapes the emotional components of pain. Given the presence of opioid receptors in the central nucleus (CeA) of the amygdala, it has been postulated that this area also contributes to pain control through opioid mechanisms.
The descending pain modulation circuit, comprising rACC/PAG/RVM
The descending pathways that modulate pain are activated by pharmacological molecules, but also by the psychosocial context. This has been observed in placebo studies, which have effects similar to those of the drug.19
It has been observed that the placebo activates the same receptors and biochemical pathways as the drug and is therefore capable of producing a change in neuronal activity. In particular, placebo administration induced activation of three important brain regions: the dorsolateral prefrontal cortex (DLPFC), the rostral anterior cingulate cortex (rACC) and the periaqueductal grey (PAG), suggesting that the descending rACC/PAG/RVM pain modulation circuit is involved in placebo analgesia.19
However, the positive expectation associated with the placebo unifies the various stimuli, including sensory and social stimuli, within the broader psychosocial context in which we exist. The evidence suggests that positive verbal suggestions play a significant role in inducing positive expectations in patients and have an analgesic effect.
Verbal suggestions have been observed to activate not only opioid receptors (mu receptors, specific for morphine), but also CB1 endocannabinoid receptors, the cyclooxygenase pathway (aspirin-NSAIDs) and dopamine receptors. This is achieved with a duration, variability and magnitude of effect that may be less than that of drugs.20
Given that words and drugs both emerged during the course of evolution, it is more accurate to suggest that drugs operate via the same mechanisms as words.
Furthermore, in this field of enquiry, it is noteworthy that recent studies employing magnetic resonance imaging have demonstrated a correlation between thalamic activation and functional thalamus-PAG connectivity and the formation of positive memories.
The authors observed that the thalamus plays a pivotal role in the functional link between nostalgia and pain. This indicates the potential for a memory-induced analgesic modulation mechanism. The results demonstrated that the nostalgia paradigm markedly diminished the perception of pain, particularly in the case of noxious thermal stimuli.21
The effect of reducing the perception of pain was linked to the viewing of nostalgic images, including those of a bicycle used during childhood, scenes from childhood such as the old schoolyard, a candy that was popular among children at the time, or an old game from the days when they were children. The smell of childhood biscuits was also used. The researchers induced the secretion of substances that lowered the perception of pain, including serotonin, noradrenaline and endorphins.
Given its predominantly positive valence, nostalgia therefore performs an analgesic function by activating neuronal pathways that have been shaped by evolutionary processes.
Pain modulation hypotheses: social and cultural factors
Pain modulation is influenced by social factors.22
Socio-familial and ethnic context have been identified in the literature as relevant factors in the determination of pain perception.
The relational-familial context in which a child lives has been identified as a significant factor influencing the perception of pain threshold.23 It has been observed that the pain and fear experienced by children during venous punishment are related to the parents' ability to regulate emotions.
Indeed, the latter enact a series of behaviours that direct the child's attention towards the procedure and inadvertently communicate anxiety, fear or their own concerns.
Thus, the factors that influence the child's perception of pain appear to be related, in various ways, to parental behaviour according to their ability to regulate emotions, with the effect of amplifying or reducing the perception of paediatric pain.24
Pain perception and response can be strongly influenced by cultural and ethnic differences.
Some populations, for example the Zulu and Aboriginal communities (South Africa and Australia) are better able to tolerate pain and especially to experience less of it.
Their expectation towards back pain and towards pain in general is positive.
They therefore have a completely different approach to pain than the peoples of the western world, who tend to stay at rest and be afraid to move around, and reject pain as a disease.25
We then see how social determinants can positively or negatively influence the perception of pain.
In an integrated statistical analysis of 1,191 women with early-stage breast cancer treated at a large cancer centre in Memphis, Tennessee, it was observed that pain is the most common side effect of breast cancer.
The study showed that adequate pain management is crucial to support treatment tolerance.26-27 Patients' quality of life is therefore an important element in improving cancer treatment.27 Pain among women with breast cancer was observed to be significantly associated with stress.28 Socially isolated patients had a higher risk of breast cancer mortality than socially integrated patients.29-30
Social determinants also showed a significant association with pain perception.31
Women who lived in poorer neighbourhoods were likely to have undertreated pain.
It could be deduced from these studies that both the management of post-diagnosis pain in the breast cancer patient and the patient's own care plan must take into account not only pathological factors but also social conditions that allow better pain and disease management.32
Hypotheses about pain modulation in relation to relationships with others
It is also worth noting the results of recent studies that have investigated the influence of social relationships on the perception of pain.
In particular, studies conducted by Wang et al. showed that the subjective experience of pain can be altered when an individual decides to help another person.
Neuroimaging studies have shown that prefrontal regions (e.g. the dorsolateral prefrontal cortex [DLPFC]) and areas associated with the affective processing of pain (the amygdala) modulate the effects of pain anticipation on subjective evaluations.33-35
Furthermore, the PAG is widely recognized for its role in modulating pain in this type of social feedback situation.
The act of helping others, whether by donating resources to a stranger or the bearing someone else's suffering, has been found to have a beneficial outcome.
At the neural level, the altruistic condition (as opposed to the control condition) led to a reduction in the response to painful stimuli in pain-related brain areas.40
Discussion and Conclusion
In light of the aforementioned considerations, following an analysis and evaluation conducted by a Task Force of international experts, the IASP has reformulated the definition of 'Pain' (Pain 23 May 2020).
This latter interpretation appears to align with the Greek etymology of 'ποινή', which permits a re-evaluation of pain in its multidimensional form.
Pain is not merely a transduction of impulses associated with a pathogenic noxa and transmitted through the nervous system, where it alters its plasticity. Rather, pain represents a personal experience.
The biopsychosocial model (BPS) represents an evolution of the biomedical model, which employs pharmacological and/or minimally invasive treatments. This model may offer a promising avenue for enhancing disease management and quality of life for individuals with pain and their families.
By centring the patient within the context of their social environment, each treatment pathway can be tailored to the individual, potentially leading to more effective pain and disease management.
Conflict of interests
The authors declares no conflict of interests
Open Access-license (CC BY-NC 4.0)
{kind=link}
Published
30th October 2024
Bibliografia
1) Hudspith MJ. Anatomia, fisiologia e farmacologia del dolore. Anaesth Terapia Intensiva Med 2019;17(9):425–430.
2) Nikolenko VN, Shelomentseva EM , Tsvetkova MM, Abdeeva EI et al. Nociceptors: Their Role in Body’s Defenses, Tissue Specific Variations and Anatomical Update. Journal of Pain Research 2022;15 867-877_https://doi.org/10.2147/JPR.S348324
3) Frias B, Merighi A. Capsaicin, Nociception and Pain Molecules 2016; 18;21(6).
3) Frias B, Merighi A. Capsaicin, Nociception and Pain Molecules 2016; 18;21(6).
4)Tracey WD. Nociception.Curr Biol. 2017; 20;27(4):R129-R133.
5) Woller SA, Eddinger KA, Corr M, Yaksh TL. An overview of pathways encoding nociception. Clin Exp Rheumatol;35 Suppl 107(5):40-46.
6) Scott A. Armstrong; Michael J. Herr. Physiology, Nociception In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan May.
7) Roma Pahwa; Amandeep Goyal; Ishwarlal Jialal. Chronic Inflammation 2022; StatPearls Publishing LLC
8) Bonezzi C, Fornasari D, Cricelli C, Magni A, Ventriglia G. Not All Pain is Created Equal: Basic Definitions and Diagnostic Work-Up. Pain and Therapy 2020; 9: 1–15. Nature Reviews Disease Primers volume 5, Article number: 41 (2019)
9) Zhou, HY, Chen SR, Pan HL. TargetingN-methyl-D-aspartate receptors for treatment of neuropathic pain. Expert Rev. Clin. Pharmacol. 2011, 4, 379–388.
10) Vranken JH. Meccanismi e trattamento del dolore neuropatico. centesimo. Nerv. Sist. Agenti Medi. Chim. 2009; 9 :71–78. doi: 10.2174/187152409787601932.
11) Suk-Yun Kang, Su Yeon Seo, Se Kyun Bang, Seong Jin Cho, Kwang-Ho Choi, and Yeonhee Ryu. Inhibition of Spinal TRPV1 Reduces NMDA Receptor 2B Phosphorylation and Produces Anti-Nociceptive Effects in Mice with Inflammatory Pain. Int J Mol Sci. 2021; 22(20): 11177.
12) Moore KA, Kohno T, Karchewski LA, Scholz J. Partial peripheral nerve injury promotes a selective loss of GABAergic inhibition in the superficial dorsal horn of the spinal cord. The Journal of Neuroscience. 2002;22(15):6724–6731.
13) Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW et al Neuropatia diabetica. Primer Nat Rev Dis.2019;5(1):41.
14) Harasawa I, Joshua PJ, Fields HL, Porreca F, and Meng ID. Alterations in the rostral ventromedial medulla after the selective ablation of μ-opioid receptor expressing neurons. Pain 2016; 157(1): 166–173. doi: 10.1097/ j.pain .0000000000000344
15) Zhang Y, Zhao S, Rodriguez E, et al. Identifying local and descending inputs for primary sensory neurons. J Clin Invest, 2015. 125(10): p. 3782-94.
16) Gao YJ, Ren WH, Zhang, YQ, Zhao ZQ et al. Contributions of the anterior cingulate cortex and amygdala to pain- and fear- conditioned place avoidance in rats. Pain, 2004. 110(1-2): p. 343- 53.
17) Zhang LY, Zhang, and Z.Q. Zhao, Anterior cingulate cortex contributes to the descending facilitatory modulation of pain via dorsal reticular nucleus. Eur J Neurosci, 2005. 22(5): p. 1141-8.
18) Ren K, A. Randich and GF Gebhart. Electrical stimulation of cervical vagal afferents. I. Central relays for modulation of spinal nociceptive transmission. J Neurophysiol, 1990. 64(4): p. 1098-114.
19) Frisaldi E, Shaibani A, Benedetti F. Understanding the mechanisms of placebo and nocebo effects. Swiss Med Wkly. 2020;150:w20340.Publication Date: 01.09.2020
DOI: https://doi.org/10.4414/smw.2020.20340.
20) Benedetti F. L’effetto placebo. Breve viaggio tra mente e corpo. Carocci editore 2018.
21) Zhang M, Yang Z, Zhong j, ZhangY, et al. Thalamocortical Mechanisms for Nostalgia-Induced Analgesia. J Neurosci 2022; 6;42(14):2963-2972.
doi: 10.1523/JNEUROSCI.2123-21.
22) Raffaeli W, Chiadini A. Dare un nome al Dolore. Il cammino di Fondazione Isal trent’anni di storia NFC edizioni 2022.
23) La Magra I. Soglia del dolore: i fattori che influenzano la percezione del dolore nel bambino. PNM 2015; 2.
24) Constantin KL, Moline RL, Pillai Riddell R, Spence JR et al. Biopsychosocial Contributors to Parent Behaviors during Child Venipuncture. Children 2022, 9, 1000. https://doi.org/10.3390/children9071000
25) I B Lin, P B O'Sullivan, J A Coffin, D B Mak, S Toussaint, L M Straker ‘I am absolutely shattered’: The impact of chronic low back pain on Australian Aboriginal people. Eur J Pain 2012;16(9):1331-41.doi: 10.1002/j.1532-2149.2012.00128.x. Epub 2012 Mar 6.
26) Willey C, Silliman RA. The Impact of Disease on the Social-Support Experiences of Cancer Patients. J Psychosocial Oncol (1990) 8:79–95. doi: 10.1300/J077v08n01_06 - DOI
27) Montazeri A. Health-Related Quality of Life in Breast Cancer Patients: A Bibliographic Review of the Literature From 1974 to 2007. J Exp Clin Cancer Res (2008) 27:32. doi: 10.1186/1756-9966-27-32.
28) Koopman C, Hermanson K, Diamond S, Angell K, Spiegel D. Social Support, Life Stress, Pain and Emotional Adjustment to Advanced Breast Cancer. Psycho-Oncology 1998; 7:101–11. doi: 10.1002/(SICI)1099-1611(199803/04)7:2<101:AID-PON299>3.0.CO;2-3.
29 ) Maunsell E, Brisson J, Deschěnes L. Social Support and Survival Among Women With Breast Cancer. Cancer 1995; 76:631–7. doi: 10.1002/1097-0142(19950815)76:4<631::AID-CNCR2820760414>3.0.CO;2-9.
30) Arora NK, Finney Rutten LJ, Gustafson DH, Moser R, Hawkins RP. Perceived Helpfulness and Impact of Social Support Provided by Family, Friends, and Health Care Providers to Women Newly Diagnosed With Breast Cancer. Psycho-Oncology 2007; 16:474–86. doi: 10.1002/pon.1084
31) Kawachi I, Berkman LF. Neighborhoods and Health. Oxford, England: Oxford University Press (2003).
32) Berkman LF, Kawachi I, Glymour MM. Social Epidemiology. Oxford, England: Oxford University Press (2014)..
32) Hyo Young Choi, Ilana Graetz, Arash Shaban-Nejad, Lee Schwartzberg, et al. Social Disparities of Pain and Pain Intensity Among Women Diagnosed With Early Stage Breast Cancer. Front. Oncol., 08 February 2022. Sec. Breast Cancer. https://doi.org/10.3389/fonc.2022.759272
33) Sharvit G, Corradi-Dell'Acqua C, Vuilleumier P. Modality-specific effects of aversive expectancy in the anterior insula and medial prefrontal cortex. Pain. 2018; 159:1529–42. doi: 10.1097/j.pain.0000000000001237.
34) Atlas LY, Bolger N, Lindquist MA, Wager TD. Brain mediators of predictive cue effects on perceived pain. J Neurosci 2010; 30:12964–77. doi: 10.1523/ J Neurosci.0057-10.2010.
35) Kragel PA, Kano M, Van Oudenhove L, Ly HG, Dupont P, Rubio A, et al. Generalizable representations of pain, cognitive control, and negative emotion in medial frontal cortex. Nat Neurosci 2018; 21:283–9. doi: 10.1038/s41593-017-0051-7.
36) Mills EP, Keay KA, Henderson LA. Brainstem pain-modulation circuitry and its plasticity in neuropathic pain: insights from human brain imaging investigations. Front Pain Res 2021; 2:34. doi: 10.3389/fpain.2021.705345.
37) Hemington KS, Coulombe M-A. The periaqueductal gray and descending pain modulation: why should we study them and what role do they play in chronic pain? J Neurophysiol 2015; 114:2080–3. doi: 10.1152/jn.00998.2014.
38) Wang Y, Ge J, Zhang H, Wang H, Xie X. Altruistic behaviors relieve physical pain. Proc Natl Acad Sci USA.2020; 117:950–8. doi: 10.1073/pnas.1911861117.
39) López-Solà M, Koban L, Wager TD. Transforming pain with prosocial meaning: a functional magnetic resonance imaging study. Psychosom Med 2018; 80:814–25. doi: 10.1097/PSY.0000000000000609.
40) Sharvit G, Schweinhardt P..The influence of social signals on the self-experience of pain: A neuroimaging review. Front Neurol 2022; Sec. Applied Neuroimaging. https://doi.org/10.3389/fneur.2022.856874.