Post-herpetic neuralgia: diagnosis and therapy
A clinical situation that is the synthesis
of all types of neuropathic pain
Review
Pathos 2024; 31. 1. Online 2024, Jun 30
_____________________________________________________________________________
Guido Orlandini
Pain Medicine
Villa Ravenna (Chiavari-Ge)
SYNLAB Institute (Monza-MB)
_____________________________________________________________________________
Summary
Post-herpetic neuralgia (PHN) is of particular interest to the algologist because it can be produced by all the pathogenetic mechanisms of neuropathic pain, singly or variously associated. PHN is caused by reactivation in the spinal or cranial ganglia of the varicella virus, which initiates different pathogenetic mechanisms depending on the nerve site reached: in the ganglion it involves cell body damage and deafferentation of the 2nd neuron (deafferentation PHN or type III), migrating to the skin it causes peripheral nerve damage with nerve fiber disruption (axonal neuropathy PHN or type II A) and/or demyelination of Aα, Aβ and Aδ fibers (demyelination PHN or type II B) as well as nociceptor damage (persistent nociceptor hyperexcitability PHN or type I). Finally, centripetal migration of virus towards the neuraxis results in damage to the dorsal root (Type III PHN) and central neurons (central PHN or type IV).
Riassunto
La nevralgia post-erpetica (NPH) è particolarmente interessante per l’algologo perché può essere prodotta da tutti i meccanismi patogenetici del dolore neuropatico, singolarmente o variamente associati. La NPH è causata dalla riattivazione nei gangli spinali o cranici del virus della varicella che avvia meccanismi patogenetici differenti a seconda della sede nervosa raggiunta: nel ganglio comporta il danno dei corpi cellulari e la deafferentazione del 2°neurone (NPH da deafferentazione o III tipo), migrando verso la cute provoca il danno dei nervi periferici con interruzione della fibra nervosa (NPH da neuropatia assonale o II tipo A) e/o la demielinizzazione delle fibre Aα, Aβ e Aδ (NPH da demielinizzazione o II tipo B) nonché il danno dei nocicettori (NPH da persistente ipereccitabilità dei nocicettori o I tipo). Infine, la migrazione centripeta del virus verso il nevrasse comporta il danno della radice dorsale (NPH III tipo) e dei neuroni centrali (NPH centrale o IV tipo).
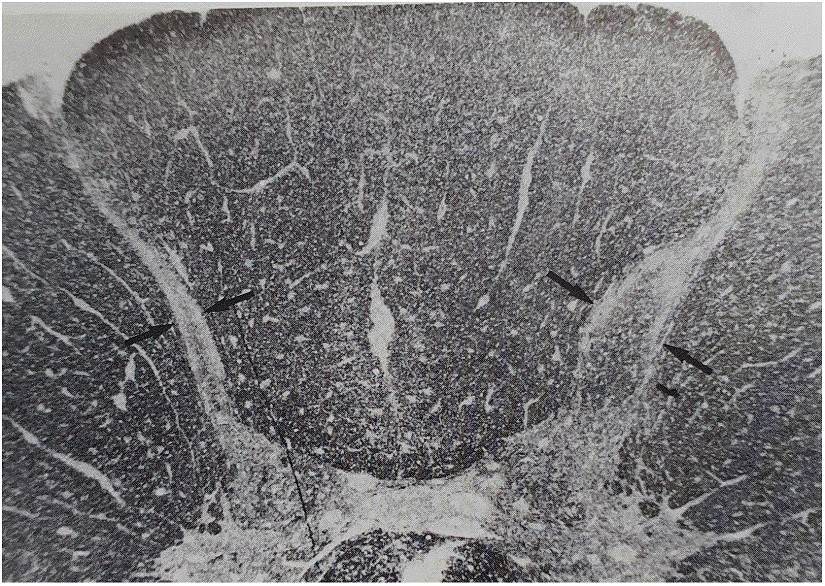
The most significant knowledge of the pathogenesis of PHN comes from anatomical findings in five patients who died of intercurrent diseases and underwent autopsy.16 Of these subjects, three had PHN at death and two had had an HZ 2 and 3 months previously, respectively (Figure 1).
Trigeminal nucleotomy
Key words
Postherpetic, neuralgia, herpes zoster, pain, neuropathic, therapies
Parole chiave
Nevralgia, post-erpetica, herpes zoster, dolore, neuropatico, terapie
Introduction
In the chapter of neuropathic pain, post-herpetic neuralgia (PHN) is a very special condition because, far from being a single entity, all the pathogenetic types of neuropathic pain are possible in it, either singly or variously represented, causing the clinical picture to vary in severity, conditioning the prognosis and complicating therapy. This is why the study of PHN is particularly interesting: it proposes various stimulating questions that make us critically reconsider our knowledge of the pathophysiology of pain, pain semeiotics and therapeutic decision-making.
Removed the simplistic belief that PHN is a single entity, it is even necessary to clarify what is meant by it. For some, PHN is any pain that remains after healing of skin lesions from Heper Zoster (HZ) i.e. 2-4 weeks and for most it is pain that persists for 3 months, 6-12 months or forever. It is clear that if we only consider PHN to be pain that persists for more than a year, its incidence is somewhat lower than if we also consider pain present just after the rash has resolved or after 3 months.
If there is approximation on the incidence of HZ (300-800 cases/100,000/inhabitants/year),1-4 there is even more on the incidence of PHN. In fact, given that in many patients the HZ infection causes symptoms that are prolonged over time to such an extent as to justify the popular expression "nine-moon evil" and that there is a tendency towards spontaneous recovery, if clear boundaries are not established between HZ and PHN, not only is it impossible to know when one ends and the other begins, but neither can the incidence of PHN be established with certainty. According to Kost and Straus 1 70% of HZ cases become PHN that heals within a year and 45% become PHN that lasts forever. For some, HZ becomes PHN in 20% of cases 5 and others speak of 33%.6 According to Paisley and Serpell,7 PHN occurs following HZ in 60% of patients over 50 years and in 75% of those over 75 years.
Finally, with regard to the site involved, the thoracic region would be affected in 55% of cases, the lumbar region in 14%, the cervical region in 12%, the sacral region in 3% and the cranial region in 15%.8,9
Clinical expression
Another element of confusion concerns the clinical expressiveness of PHN: for some, PHN is only referred to when there is pain and not when there is only allodynia, which is considered as “abnormal sensitività”, and for others even with only the presence of allodynia. In 70-80% of cases a prodromal period with pain precedes the onset of the herpetic eruption by 4-5 days: some patients have a longer prodromal period (up to 100 days) while in others there is no prodromal period and pain appears with the onset of the eruption or even afterwards. Finally, in some cases there is only pain without eruption (zoster sine herpete). In 1979 Lipton 10 summarised the clinical features of PHN by stigmatising them into the following points: 1) uniform, uretic or dysesthetic pain; 2) paroxysmal, flashing pain; 3) allodynia
Pathogenesis
A wide variety of factors have been implicated in the pathogenesis of PHN, which explains the diversity of treatments proposed and the lack of a clear correlation between them and the pathogenetic mechanism. The only universally accepted finding is that in individuals who have contracted chickenpox in childhood, the varicella-zoster virus remains nested in the sensory ganglia throughout life and its reactivation is prevented by the cellular immunity induced by the primitive infection. It is a reduction in immune defences that allows it to reactivate and resume replication. Over a lifetime, the risk of reactivation of virus with HZ production would be around 30%.11
It should be noted that the resumption of virus activity finds the immunocompetent system sensitised at the time of chickenpox, so the immune response is brisk enough to confine it to the site where it started. Hence, HZ usually affects just one metamer and its spread beyond that zone, usually with lethal outcome, only occurs in severely immunocompromised patients.
Historically, there have been numerous hypotheses to explain the pathogenesis of PHN and it is worth briefly reviewing the most significant ones because, although they are not individually exhaustive, each provide a piece to its understanding.
The input imbalance hypothesis
In 1959 Noordenbos 12 hypothesised that ganglioradiculitis produced damage to myelin Aβ fibres resulting in reduced inhibition of nociceptive afferents. The input imbalance hypothesis (intimately related to Melzack and Wall's gate-control theory) 13 is the best known of those proposed to explain the pathogenesis of PHN.
Hypothesis of ephaptic contacts
Upon infecting the rat dorsal root ganglia with HZ virus, Schon et al 14 observed that ganglioradiculitis, possibly due to the establishment of ephaptic contacts, results in a repetitive, hypersynchronous discharge of ganglion cells that may be responsible for chronic abnormal input to the medulla and thus the persistence of pain.Chronic inflammation hypothesis
PHN would be sustained by the persistence of inflammation caused by virus reactivation. In fact, in one of Watson et alautopsy findings 15 lymphocytic infiltrates with a phlogistic imprint were found in the dorsal root ganglion (DRG), and according to Devor,16 remission of the inflammation results in the abolition of foci of ectopic electrogenesis. In support of the inflammation thesis, Kim et al 17 evaluated the importance of investigating markers of inflammation (ESR, C-reactive protein and white blood cell count) as a predictor of the evolution of HZ into PHN, reporting that ESR is the most signicative marker. Moreover, recently the same Kim et al,17 observing that skin temperature changed from hot to cold 12 weeks after HZ signalling the end of the inflammatory phase, argued that only if pain is still present after 3 months can one speak of PHN. In reality, the so-called inflammatory phase can last much longer than 3 months 18 and therefore it is not clear whether it is appropriate to speak of PHN only when the inflammatory phase has resolved and permanent nerve damage remains or also when inflammation is still present and is a concomitant or in some cases even the main cause of PHN. In the first case, we are faced with PHN caused by nerve damage, with no possibility of healing that will last forever, whereas in the second case we are faced with inflammatory PHN that is treatable with methylpredisolone (intrathecal or peridural) and, if it has not produced excessive nerve damage, will resolve within a certain time (3-6-12 months).
Sympathetic Hypertone Vasoconstriction Hypothesis
According to Colding,19 ganglioradiculitis causes abnormal input on the dorsal horn of the spinal cord and the resulting sympathetic hypertone produces isosegmental vasoconstriction responsible for ischaemia, hypoxia and cell lysis. In turn, the pain thus produced maintains the abnormal input on the spinal cord and the sympathetic hypertone responsible, in a vicious circle, for chronic nociceptor activation. This thesis, which pathogenetically approximates PHN to CRPS-I according to the classical theory of Leriche and Livingston,20,21 is not entirely convincing while (without considering the vicious circle) the thesis that vasoconstriction produces ischaemic damage to nerve fibres 22 is probably valid.
According to Colding,19 ganglioradiculitis causes abnormal input on the dorsal horn of the spinal cord and the resulting sympathetic hypertone produces isosegmental vasoconstriction responsible for ischaemia, hypoxia and cell lysis. In turn, the pain thus produced maintains the abnormal input on the spinal cord and the sympathetic hypertone responsible, in a vicious circle, for chronic nociceptor activation. This thesis, which pathogenetically approximates PHN to CRPS-I according to the classical theory of Leriche and Livingston,20,21 is not entirely convincing while (without considering the vicious circle) the thesis that vasoconstriction produces ischaemic damage to nerve fibres 22 is probably valid.
The “ectopic pacemaker” hypothesis
A more recent pathogenetic hypothesis,16 is that of “ectopic pacemakers” which would be found in the axon and DRG. According to this theory, foci (microneuromas and demyelination zones) would form along the axon where ectopic activation of the fibre becomes possible either as a result of locally applied stimuli or spontaneously, which in turn is responsible for the production and maintenance of central hyperexcitability.
Ectopic pacemakers' in the axon
It has been found that in PHN there is loss of small fibres in the epidermis and this observation brings it closer to neuropathic pain from small fibre damage. The damage of the small fibres could be due to the destruction of the cell bodies in the ganglion and the consequent Wallerian degeneration of the corresponding axons, or to the phenomenon Devor calls “dying-back”, which would not depend on the destruction of infected ganglion cells but on their “metabolic stress” responsible for partial degeneration of the axon. “By 'retracting” (to use Devor's word) from the nociceptor, axon would produce microneuromas in its bundle that discharge spontaneously. The hyperexcitability would therefore not be at the expense of the nociceptors but of the microneuromas that form in the axon, proximal to nociceptors.
Ectopic pacemakers' in the DRG
In addition to ectopic electrogenesis at the distal axonal level, ectopic pacemaker thesis also considers possible ectopic electrogenesis in the DRG. Historically, DRG has been considered a possible site of ectopic electrogenesis in neuropathic pain from axonal neuropathy (along with neuroma), and it even appears that this abnormality is particularly sensitive to local anaesthetics, justifying their efficacy with systemic administration. It has even been hypothesised that if systemic administration of anaesthetics is effective, the damage is ganglionic, otherwise it is in the neuroma.
Central sensitisation
In the ectopic pacemaker hypothesis, the role of central sensitisation induced and maintained by afferents from foci of ectopic electrogenesis in microneuromas in nerve fibre terminals and ganglion cells is emphasised.
Allodynia
Another element to be considered is allodynia: if we consider a role of nociceptors as possible, it should be considered C-mediated, but in Devor's thesis an Aβ-mediated allodynia due to persistent central hyperexcitability cannot be disregarde.
Ultimately, according to the pathogenetic hypothesis of ectopic pacemakers, focus should be shifted from CNS to PNS: it would no longer be a question of deafferentation or central pain, but of peripheral neuropathic pain from activation of an ectopic electrogenesis in the axon or DRG where central hyperexcitability would function as an aggravating factor. Obviously, this view shifts therapeutic decisions towards controlling the dysfunction of the first neuron with measures such as application of medicated patches.
Hypothesis that (integrating the previous ones) is based on the site of nerve damage
Although none of the previous hypotheses explains the complex pathogenesis of PHN on its own, by taking up a few concepts and placing them in a certain sequence, one may think that ganglion phlogosis induces sympathetic hypertone and that this, in turn, causes vasoconstriction and consequently ischaemic nerve tissue damage.
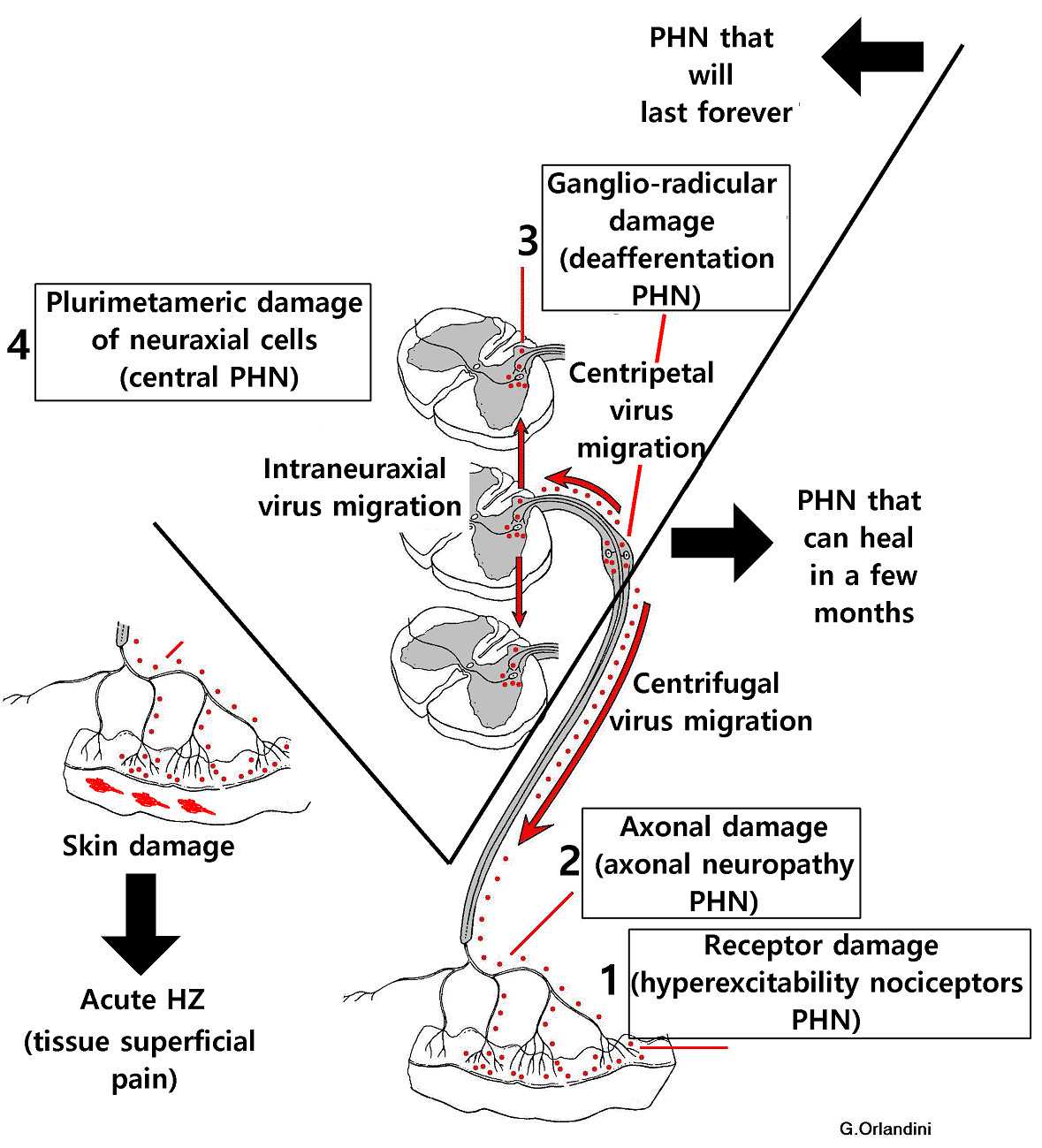
If we now introduce the concept of virus migration by axonal transport from the sensory ganglion to the neuraxis and periphery to the skin, we can assume that at each site where it arrives, virus causes inflammation which in turn initiates the “sympathetic hypertone -> vasoconstriction -> ischaemic nerve tissue damage” sequence. Consequences of the latter are different depending on the site where it manifests itself and thus one can have pain from nociceptor hyperexcitability, from axonal neuropathy, from demyelination, from deafferentation and central. From this it is clear that (in agreement with Peng et al23 when they maintain that PHN is sustained by many pathogenetic factors operating at the same time) PHN is not a single pathogenetic entity but a clinical reality where all the pathogenetic types of neuropathic pain are possible, singularly or variously represented, causing the different severity of the clinical picture and conditioning the prognosis, which may be that of a disease destined to heal or to last forever.The most significant knowledge of the pathogenesis of PHN comes from anatomical findings in five patients who died of intercurrent diseases and underwent autopsy.16 Of these subjects, three had PHN at death and two had had an HZ 2 and 3 months previously, respectively (Figure 1).
{kind=link}
Referring to the 3 cases of PHN, this study showed:
1) loss of axons and myelin in the peripheral nerve distal to the ganglion (PHN from axonal neuropathy and demyelination);
2) loss of cell bodies, axons and myelin replaced by fibrous tissue in the ganglion (deafferentation PHN);
3) loss of axons and myelin in the dorsal root (deafferentation PHN); and
4) marked atrophy in the dorsal horn of the spinal cord In addition, in one case, lymphocytic infiltrates with a phlogistic imprint were found in the dorsal root ganglion and root, which may have been responsible for a chronic inflammatory-based PHN that does not correspond to the nerve damage but could be its cause (Figure 2, Figure 3)
{kind=link}
{kind=link}
Considerations on IV Type PHN
Type IV PHN (from central lesion) deserves some considerations. Destruction of the cells of the dorsal horn of the spinal cord extended to several bordering metameres justifies the severe sensory deficit (which is not analgesia but “anaesthesia” because central lesion does not only affect the cells of origin of second nociceptive neuron but also Aβ fibres that run medially to the dorsal horn of the spinal cord to enter the DREZ) but does not cause central pain or even allodynia.
In this regard, let us recall the pathophysiology of central pain: the anatomical lesion that produces it is the isolated neo-spinothalamic bundle which, by “deafferenting” the ventro-postero-medial and ventro-postero-lateral (VPM-VPL) nuclei that normally activate the reticulo-thalamic (RT) nucleus it removes the GABA-ergic inhibition exerted by the latter on dorso-median nucleus (DM) and on VPM-VPL nuclei themselves with consequent prevalence of glutamatergic activity of paleo-spinothalamic bundle and MAS. Quite different is the anatomical damage in PHN with central lesion because it does not involve the neo-spinothalamic bundle but entails in the dorsal horn of the spinal cord the damage of the cells of origin of neo-spinothalamic bundle, paleo-spinothalamic bundle and MAS, as DREZ-lesion (Figure7).
Ultimately, what appears to be the most severe expression of PHN may instead represent its favourable evolution since the lesion that produces it is the same as the one obtained by performing the DREZ-lesion.
Why some PHN heals and others do not
Regarding the reason why some PHN resolve (even spontaneously) in 3-12 months and others do not resolve at all, the assertion that remission of inflammation results in the abolition of foci of ectopic electrogenesis 23 explains the remission of PHN sustained by peripheral (receptor or axonal) damage but to get a more complete picture, let us reason about the possibility of spontaneous remission of neuropathic pain in general. Clearly there is no remission in stump pain caused by axonal damage to all the nerve fibres of all the peripheral nerves of amputated limb, whereas there may be in lumbosacral radiculopathy, which involves axonal damage confined to a limited number of nerve fibres within the involved radicular nerve, in trigeminal neuralgia caused by foci of demyelination, and in pain from hyperexcitability of nociceptors. From the above, we deduce that remission of neuropathic pain is possible in some pathogenic types and not in others. Applying this rule to PHN, one may think that remission is possible depending on the prevailing type of neuropathic damage that sustains it. PHN may recede in a few months if it is sustained by receptor damage (Type I PHN), axonal damage or myelin damage (Type II PHN) but not if it is sustained by deafferentation (Type III PHN).
Diagnosi
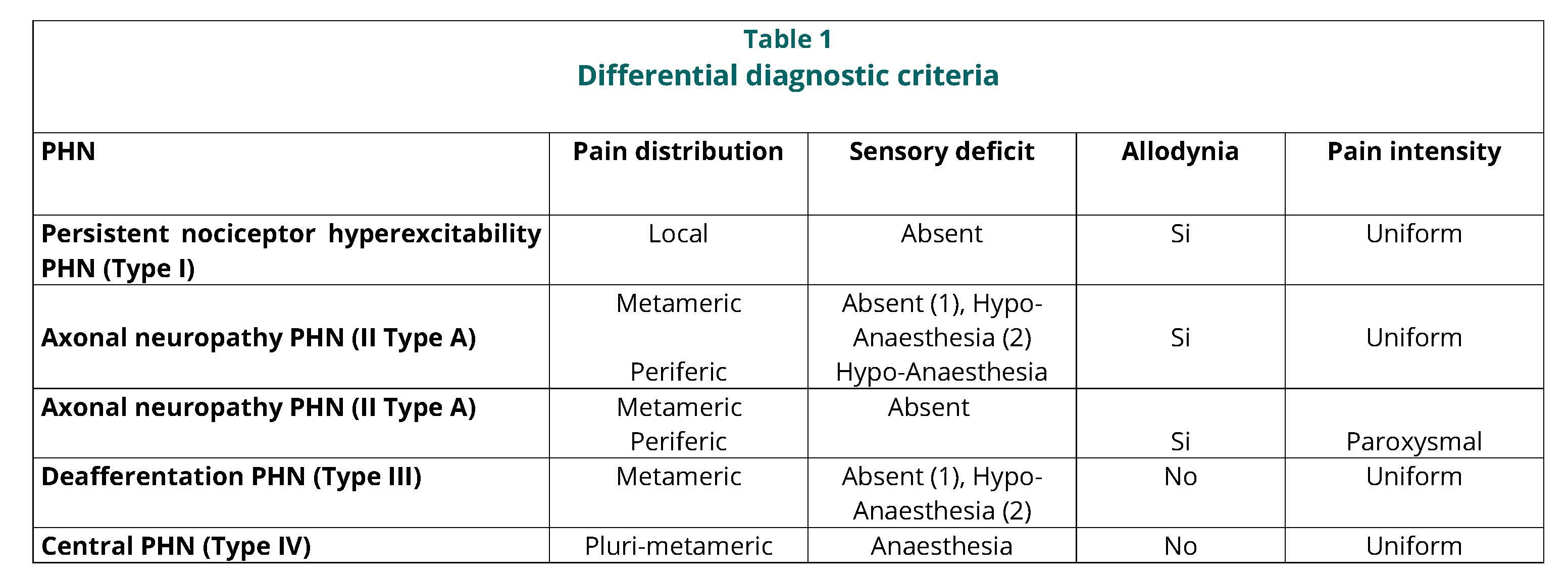
Clinically, to recognise the pathogenic type of PHN, we can refer to a number of criteria, which are: topographical distribution of pain, presence and type of sensory deficit, presence of allodynia and character of the pain intensity pattern (Table 1).
{kind=link}
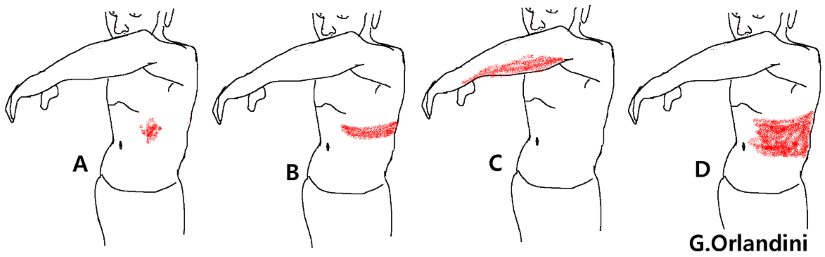
It is worth starting the diagnostic reasoning from the criterion of the topographical distribution of pain, which can be local (area that follows the distribution of the tissue lesion), metameric (area that corresponds to the peripheral receptor field of a radicular nerve or nerve root), peripheral (area that corresponds to the receptor field of a peripheral nerve) or plurimetameric.
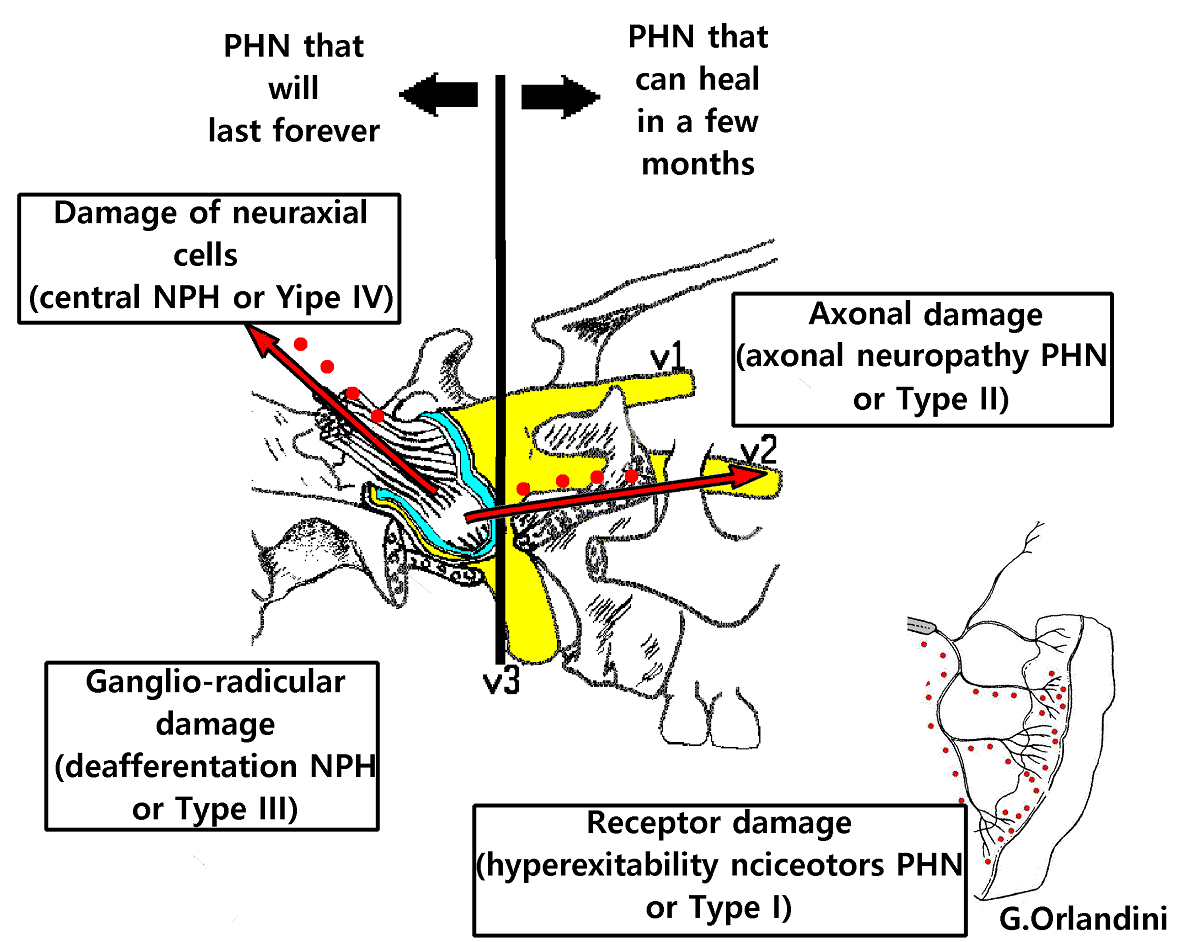
If the topographic distribution of pain is metameric, it is Type II or III PHN (Figure 4). In the case of spinal nerves there is no sensory deficit because the uninjured nerves above and below pick up information from the territory of the damaged one; instead, in the case of trigeminal nerves, there may be hypo-anesthesia because each trigeminal territory is innervated by only one branch without overlapping. Allodynia is present in Type II PHN and not in Yype III PHN. In axonal neuropathy PHN, dynamic (Aβ-mediated) allodynia depends on the pathological excitation of the second neuron by the Aβ fibres which, as a compensatory phenomenon, have proliferated following the transganglionic degeneration of C fibres resulting from neurite damage. In the case of demyelination PHN, dynamic (Aβ-mediated) allodynia depends on the same mechanism that produces it in trigeminal neuralgia where the tactile stimulus activating the Aβ fibres causes presynaptic depolarisation of C fibres inducing their massive discharge and paroxysmal pain.24
{kind=link}
Allodynia is absent in Type III PHN (deafferentation PHN) because Aβ fibres are missing. In deafferentation pain there is no allodynia because, if there were, it would have to be Aβ mediated, since there is no reason for it to be C mediated. However, if there is Aβ-fibre activity, there may be deafferentation but no deafferentation pain and if there is deafferentation pain it means that there is no Aβ-fibre activity.
Finally, if the topographic distribution of pain is plurimetameric, it is Type IV PHN (Central) which is associated with anaesthesia without allodynia because there are no C or Aβ afferents capable of causing it.
Prevention of herpes zoster
HZ can only be prevented by vaccination. There are two types of anti-Zoster vaccine: one consists of attenuated viral cells ("zoster vaccine") 25,26 and another ("recombined vaccine") contains an antigen of virus together with an adjuvant called ASO1B (sic). Note that it has been repeatedly reported that “zoster vaccine” is contraindicated in immunocompromised individuals,26 i.e. those who need it most, whereas Shingrix would not have this contraindication.27
With regard to efficacy, one of the first studies,28 that included 38546 subjects over the age of 60 who were randomly vaccinated with either the zoster vaccine or placebo showed that over an average observation period of 3 years, 957 contracted HZ (315 vaccinated and 642 unvaccinated) and 107 contracted PHN (27 vaccinated and 80 unvaccinated): in practice, vaccination reduced the incidence of HZ by 51% and the incidence of PHN by 66%. These data were later confirmed by Arnold and Messaoudi26 and then by Klein et al,28 stating that the efficacy of the "zoster vaccine" was 65% with "moderate" efficacy for 8 years.
Subsequent studies have shown even better results, in fact according to Cunningham et al,29 the “recombinant vaccine” would reduce the chance of contracting HZ by 91% and of contracting PHN by 88%, and according to Izurieta et al,30 administered in two doses 2-6 months apart would give 70% protection for at least 4 years. Mild and transient skin reactions at the inoculation site, myalgia and fatigue are reported as adverse effects. In addition, Shingrix would not be contraindicated in immunocompromised individuals and is preferable to the attenuated HZ virus vaccine.12 in this respect.
A recent literature review,31 analysing 22 studies involving a total of 9,536,086 subjects found that the efficacy in preventing HZ would be 45% for the "zoster vaccine" and 79% for the "recombined vaccine". All in all, vaccination significantly reduces the incidence of HZ and thus of PHN.
Treatment of herpes zoster and prevention of postherpetic neuralgia
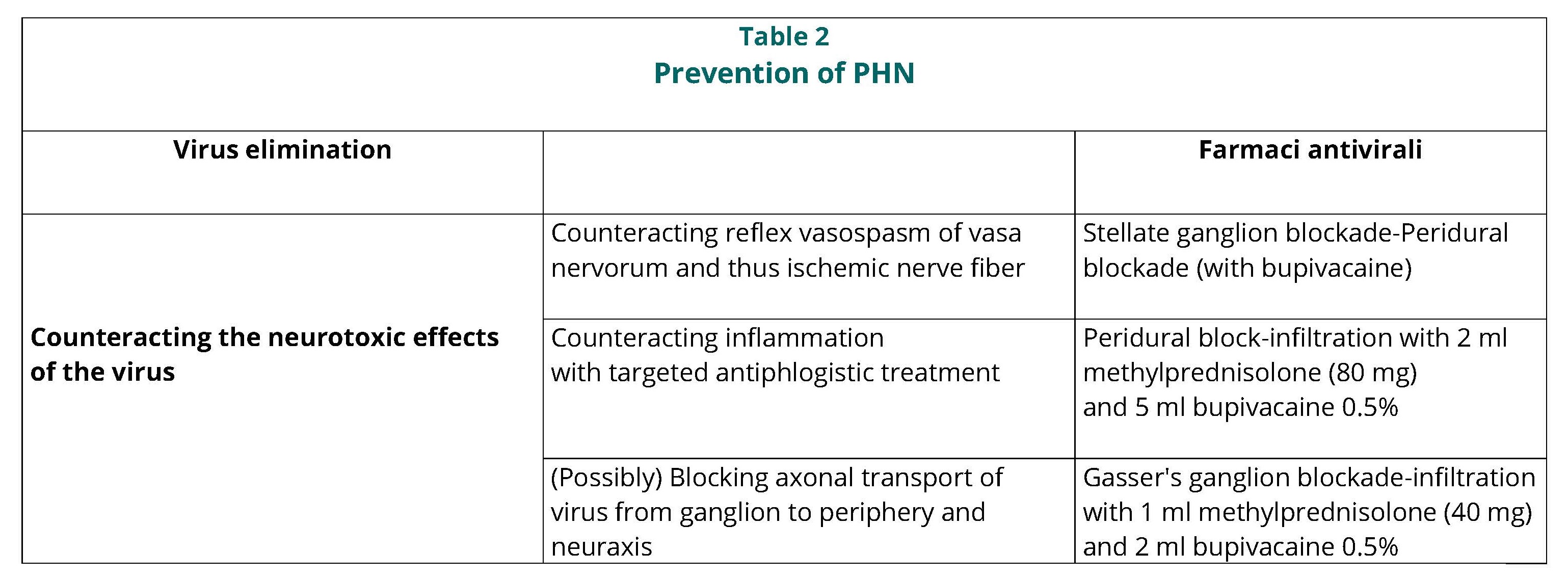
In less severe situations, especially in young subjects, systemic analgesic therapy with NSAIDs and minor opiates such as tramadol and tapentadol is sufficient, while in other cases (unfortunately limited to HZ affecting spinal nerves) “continuous epidural administration” (via elastomeric pump) of 5 mg/day of morphine for 10-15 days may be appropriate. In any case, analgesic therapy should be combined with antiviral treatment with acyclovir (cp 400-800 mg, 1cp/6 hours for 7 days) and in older patients with the prevention of PHN with measures that focus not only on eliminating the virus with antiviral drugs, but also on counteracting its neurotoxic effects (Table 2).
{kind=link}
With regard to antivirals, Herbort et al32 stated that high doses of acyclovir prevent trigeminal PHN in the first branch and that this treatment “marks the end of the corticosteroid era”! On the contrary, according to a review of the literature,33 acyclovir and famciclovir alone do not reduce the incidence of PHN, so it is necessary to proceed simultaneously with counteracting the neurotoxic effects of virus, which can be achieved: 1) by controlling reflex vasospasm of vasa nervorum and thus ischaemic damage to nerve fibres; 2) by controlling the inflammation with targeted antiphlogistic treatment; 3) by blocking axonal transport of virus from ganglion to periphery and to neuraxis.
Counteracting the neurotoxic effects of virus by controlling reflex vasospasm of vasa nervorum
The control of reflex vasospasm of vasa nervorum serves to prevent ischaemic damage to nerve tissue and can be implemented with sympathetic blockade (stellate ganglion blockade, only in the territory of the upper limb) or, at the same time as the afferent block, with the peridural block with local anaesthetic.
According to Colding,19 who was the historical initiator, based on his experience with 243 HZ patients, sympathetic blockade was effective in preventing PHN if performed very early while it had no efficacy in treating PHN. Colding's experience was confirmed by Bauman,34 who treated 38 HZ patients from 8 days to 3 months with stellate ganglion blockade (10 ml bupivacaine 0.25%) or peridural blockade (5-8 ml bupivacaine 0.25%, thus relying on the sympathetic blockade effect). At a follow-up of 6-30 months, all patients treated within 4 weeks and none of those treated later achieved complete pain control. Dan et al 35 treated 700 patients with HZ and 300 with PHN with peridural blockade (with mepivacaine 1%) and obtained a complete result (preventing PHN) in 88% of 467 patients treated within two weeks, a partial result in 96 patients treated within one month and no result in those treated later, confirming Colding's conclusions. Tenicela et al 36 treated 10 patients with sympathetic blockade and 10 with placebo, obtaining pain relief in 90% of the former and 20% of the latter. Winnie,37 examined the result in 122 patients treated with sympathetic blockade and found that in 80 % of those treated within 2 months PHN was prevented while the results in those treated later were unsatisfactory. Of particular interest is the work of Winnie and Hartwell,22 where it is stated that sympathetic blockade is effective in resolving HZ pain and preventing PHN if it is performed within 2 months of disease onset because it restores intraneural blood flow by preventing ischaemic damage to nerve fibres: if blockade is performed later it is useless because nerve damage is now irreversible.
Less exciting are the observations of Wu et al,38 who claimed that sympathetic blockade reduces the duration of pain in acute phase of HZ but it is unclear whether it prevents PHN and of Yanagida et al 39 who, after treating 49 patients (in a few cases even before the onset of HZ on the basis of clinical suspicion and in any case within the first 10 days after the rash) with stellate ganglion blockade repeated daily for 4 weeks or with peridural blockade, found that there was no result as far as preventing PHN was concerned.
Counteracting the neurotoxic effects of virus through targeted antiphlogistic treatment
Targeted antiphlogistic treatment consists of:
1) Segmental peridural blockade-infiltration with 2 ml methylprednisolone (80 mg) and 5 ml bupivacaine 0.5%, repeated after 2 weeks;
2) Gasser's ganglion blockade-infiltration with 1 ml methylprednisolone (40 milligrams) and 2 ml local anaesthetic (bupivacaine 0.5%), according to the scheme proposed by Pernak and Erdmann,40 modified for the addition of bupivacaine.
Efficacy of infiltrating Gasser's ganglion with methylprednisolone for prevention of trigeminal PHN was strongly supported by Pernak and Erdmann40 who treated 535 patients with trigeminal HZ by injecting 80 mg methylprednisolone into Gasser's ganglion. At one month after treatment 96.5 per cent of treated patients were pain-free and without analgesic support: there were only 19/535 failures (3.5 per cent) involving patients treated after the second week after the onset of HZ. Based on these results, Pernak and Erdmann recommended infiltration in the first two weeks: note also that they did not use local anaesthetic, relying only on the anti-inflammatory effect to prevent nerve damage.
It is not clear whether Pernak and Erdmann performed the infiltration of Gasser's ganglion with methylprednisolone in the trigeminal cistern or laterally in Gasser's ganglion. In this regard, a few years ago I wrote 41"...in order to perform in the treatment of trigeminal herpes zoster pain and, for what it may be worth, in the prophylaxis of post-herpetic neuralgia a treatment analogous to that practised at the spinal level with the segmental peridural block, at the trigeminal level one must not reach the cistern: this would make an inadvisable subarachnoid administration of steroid. Instead, it is necessary to administer the anaesthetic-steroid solution in the extradural space anterolateral to Gasser's ganglion...” with a procedure similar (I now add) to that used in percutaneous compression of Gasser's ganglion. Basically, introducing the needle into the cheek 1 centimetre lateral to the labial commissure and just above its horizontal plane, one directs it towards the outer 1/3 of the foramen ovale. This entry, which is very different from that required to reach the trigeminal cistern and retrogasserian root, allows the needle to be directed along a trajectory anterolateral to Gasser's ganglion which favours its extradural positioning. At this point, while to perform percutaneous compression of Gasser's ganglion one must stop the needle just beyond the entrance to the foramen ovale, in the case of anaesthetic-steroid administration one advances it 3-5 millimetres beyond the foramen ovale.
Counteracting the neurotoxic effects of virus by blocking axonal transport of virus (a controversial topic)
The first report on the use of peridural blockade to prevent PHN is that of Perkins and Hanlon42 who, having treated 12 HZ patients with bupivacaine and methylprednisolone by the peridural route, found that the treatment was effective if implemented within 7 weeks and no later than 3 months and, emphasising the key role of local anaesthetic, pointed out that the addition of methylprednisolone added nothing to the result.
Very explicit in this regard are the studies by Follini 6 and Follini and Leccabue 43 who treated 96 patients with HZ with a single, rarely repeated selective peridural block (combining the local anaesthetic with a depot steroid preparation) and found an incidence of PHN of 3.8% in patients treated within the first 2 weeks and 13 and 33.3% respectively in those treated in the third and fourth week. Similar conclusions were reached in 1999 by Hwang et al.44 A very interesting and significant contribution is made by the work of Pasqualucci et al,45 who found that after one year, 51/230 patients (22.2%) treated with intravenous acyclovir and steroids and 4/255 (1.6%) patients treated with peridural anaesthetic-steroid blockade still had pain, concluding that this procedure is more effective than intravenous administration of acyclovir and prednisolone. Further confirmation is provided by the work of Kumar et al 46 who, analysing 21 studies on the subject, concluded that there was grade A evidence that, performed within 2 months of the onset of zoster, peridural blockade with local anaesthetics and steroids reduces the incidence of PHN after one year.
Less exciting in this respect, however, are the results of a multicentre study called PINE, which is short for Prevention by epidural Injection of postherpetic Neuralgia in the Elderly.47-50 The study included 598 patients with HZ for less than 7 days treated with antivirals, analgesics and a single peridural administration of 80 mg methylprednisolone and 10 mg bupivacaine or, as a control, with antivirals and analgesics alone: at 1 month after treatment 48% of those treated with the peridural and 58% of those in the control group had pain; at 3 months 21% of those treated with the peridural and 24% of those in the control group had pain; and at 6 months 15% of those treated with the peridural and 17% of those in the control group had pain. Obviously, the Authors concluded that peridural treatment is not effective in preventing PHN. However, it should be noted that the Authors administered 10 mg bupivacaine together with 80 mg methylprednisolone (2 ml), i.e. 2 ml: it is possible that the dosage of bupivacaine was insufficient to obtain the blockade of axonal transport and that therefore the only predictable effect was that of methylprednisolone. Later, the role of peridural blockade in preventing PHN was denied by Loeser 51 and reconfirmed by Kim et al.52
Finally, we recall that in recent guidelines 53 peridural blockade with local anaesthetic and steroids is recommended especially in the first 3 weeks after the onset of HZ to prevent PHN and that recent studies supporting this procedure include that of Beydoun et al.3
In order to understand the rationale for the blockage of axonal transport we must assume that the spread of virus from ganglion towards the skin and into neuraxis continues in both directions for several days. It is obvious that when the rash occurs because a sufficient amount of viral particles have reached the skin by travelling along neuritis, a certain amount of those particles have already reached neuraxis as well: therefore blockade of axonal transport should serve to prevent other viral particles from reaching neuraxis or periphery in addition to those that have already arrived there, and this is why the infiltration is only meaningful in the first few days after the appearance of herpetic rash. In theory, the peridural or Gasser's ganglion block should be performed even before the rash appears but this is impossible because the diagnosis has not yet been made. However, if one waits too long, virus has by now reached neuraxis and peripheral branches in such quantities that blocking axonal transport is useless: therefore, with these objectives in mind, one must conclude that these procedures should be performed as soon as possible, even in the case of suspected HZ, and that every day of waiting is time allowed for viral migration.
There is no doubt that this method of preventing PHN sounds very attractive, but there is an argument that casts doubt on it: if the local anaesthetic really does block the axonal transport of virus for many days, it could simultaneously also block the transport of the trophic factors produced in the pyrenophore that maintain cell trophism and thus could cause degeneration of the nerve fibre! Actually, we know that local anaesthetic has no neurotoxic effects.
Not finding an answer in the literature and without resolving the doubt, I considered the observation that etidocaine has the same potency as tetracaine as a blocker of axonal conduction but 5 times less potent as a blocker of axonal transport, and that mepivacaine, bupivacaine and lidocaine are equally active in producing blockade of axonal conduction and axonal transport.54. Furthermore, in searching for the mechanism by which anaesthetics block rapid axonal transport, Lavoie et al. 55,56 stated that concentrations of 14-20 mM lidocaine do not produce microtubule destruction.
In this uncertainty as to the mechanism of action, it should be borne in mind that in the practice of peridural block-infiltration or Gasser's ganglion for the treatment of HZ and the prevention of PHN, local anaesthetic alone has never been used but always the combination of local anaesthetic and steroid 3,6,44,46,47,53 and by Pernak and Erdmann 40 even the steroid alone. All in all, it seems a good rule to combine steroid with local anaesthetic in all cases, relying on the antiphlogistic effect and “possibly” that of blocking axonal transport.
Therapy of postherpetic neuralgia
As I wrote about CRPS-I 41 “the less is known about a pathology, the more therapeutic proposals increase. In trigeminal neuralgia, the therapeutic options (at least the correct ones) are few because they are pathogenetically effective”: here, on the other hand, they are a huge number because they are pathogenetically unrelated and often ineffective, not to mention the space this therapeutic approximation leaves for magicians and healers. Even today, at a popular level, there is a widespread custom of relying on “marking”, which consists of tracing cross marks on the affected area “with the right hand wet with holy water” or applying crucifixes to it... preferably silver ones.
Leaving aside folk medicine, according to Aggarwal et al,57 the choice of therapy depends on the area involved and may include blockade or neurolysis of the intercostal nerves, blockade of the stellate ganglion, paravertebral neurolysis, peridural steroid injection, radiofrequency ablation of the dorsal root ganglion and if all fail, SCS...but...”in experienced hands”. In many studies, gabapentin, pregabalin, carbamazepine, amitriptyline, norpriptyline, doxepine, tramadol, lidocaine pach 5%, capsaicin, tramadol and...other opiates are generically and uncritically recommended.58-64
According to a delirious study which I do not recommend reading, it appears that, when used singly, botulinum toxin subcutaneously and pulsed RF treatment are the most effective treatments for the treatment of PHN and that, as combination therapies, the most effective is pulsed RF treatment combined with nerve block and, next, subcutaneous lidocaine infiltration combined with nerve block and ozone therapy.65
There is no shortage of suggestions deduced from literature reviews such as that of Lin et al,66 who on the basis of an analysis of a series of randomised controlled trials deduced three confusingly all-inclusive sequential lines of treatment: (1) tricyclic antidepressants, pregabalin, gabapentin and lidocaine patches; (2) tramadol and capsaicin; (3) TENS, botulinum toxin, cobalamin, triamcinolone injections, intrathecal methylprednisolone, intrathecal midazolam, stellate ganglion blockade, ganglion electrostimulation, dorsal root ganglion destruction, Pulsed RF treatment.
Of particular interest is the recent guideline drawn up by Gross et al 53 which, although it does not illustrate the pathogenetic mechanisms of PHN, deals with many clinical aspects concerning the various complications of herpetic infection: the very serious systemic dissemination of virus, meningoencephalitis, the ocular complications of trigeminal involvement of the first branch, i.e. conjunctivitis, keratitis, uveitis and even oculomotor paralysis. In these guidelines, vaccination with Shingrix administered in 2 doses 2 months apart is strongly recommended, which would provide protection against herpetic infection in 90% of cases for up to 9 years. As for therapeutic suggestions, in the acute phase of HZ the administration of antivirals (Acyclovir per os or by venous route for 10-14 days) and systemic analgesics (unfortunately) following the WHO therapeutic scale with the addition of antiepileptics (gabapentin and pregabalin) and antidepressants (especially amitriptyline) is recommended “to combat the neuropathic component of pain”. If in these guidelines the therapy proposed for HZ is rather disappointing, the advice regarding the treatment of PHN is more interesting. In particular, it is stated that lidocaine 5% patches are not a treatment of first choice while peridural blockade with local anaesthetic and steroids is strongly recommended, especially in the first 3 weeks after the onset of HZ to prevent PHN.
The problem is that all these suggestions are based on the assumption that PHN is a single entity: they are therefore not each directed against a specific pathogenetic mechanism and their efficacy is “strangely” variable. Furthermore, bear in mind that many treatments may appear to be effective because PHN often heals spontaneously. Among the few reports on the appropriateness of differentiating between various categories of PHN are the observations of Fields, Rowbotham and Baron,67 who argued that PHN could be due to abnormal sensitisation of C-fibres (nociceptor hyperexcitability PHN), damage to C-fibres (axonal neuropathy PHN) or deafferentation (deafferentation PHN) and more recently the interesting approach proposed by Forstenpointner et al 68 who, noting that patients with PHN can present with different signs and symptoms, suggested the desirability of better “identification of the sensory phenotype” of patients in order to decide on a targeted therapy.
Finally, in order to emphasise how misleading the information the public gets from Internet can be, it is stated that “...the shingles virus can be limited in its manifestations thanks to the vaccine, which must be administered within 72 hours of the onset of symptoms (the skin rush). This can alleviate both the severity and duration of complications, such as post herpetic neuralgia...which must be treated with acupuncture”.
Subcutaneous infiltration of local anesthetics and sterodes, medicated patches and capsaicin
The earliest reports on these treatments are those of Epstein,69 who advocated the efficacy of intradermal infiltration with triamcinolone for the treatment of PHN and that of Riopelle and Coo,70 where they pointed out that infiltration of local anesthetics controls pain of acute phase HZ but does not prevent PHN. Whereas Jaipur is a city in India, subcutaneous infiltration of a solution containing xylocaine 2%, bupivacaine 0.5% and dexamethasone, called "Jaipur block," was proposed in 1998. The solution was later modified by replacing dexamethasone with methylprednisolone. In the Bhargava et al,71 experience, 3960 patients with PHN present from 2 months to 5 years were treated. 96% of patients achieved complete pain control (28% after the first administration, 57% after the second, and 11% after the third): only 4% of patients did not respond to treatment. In the experience of Puri,72 30 patients with PHN were treated. 90% of patients achieved complete pain control (20% after the first administration, 60% after the second, and 10% after the third): only the remaining 10% of patients (with PHN for more than 2 years) did not respond to treatment. In the experience of Sharma et al,73 52 patients with PHN for 12 months were treated: in 50/52 patients (96%) there was a reduction of VAS from 8 to 2 achieving a satisfactory result and only in 2/52 (4%) there was no result. Nguyen et al,74 argue that subcutaneous injection of methylprednisolone and lidocaine repeated daily for 10 days can be effective of PHN. In this case, it may be thought that systemically methylprednisolone resolves the inflammation as Kotani et al,75 state referring to intrathecal administration. The observation of Mashhood,18 about the fact that lidocaine and triamcinolone infiltration is more effective than lidocaine infiltration alone in the treatment of PHN should still be mentioned. As a substitute for subcutaneous infiltration of local anesthetic, Ngo et al,5 recommended bupivacaine spray, and at the same time the application of medicated patches became very popular. Liu et al,76 recommended the use of topical drugs (lidocaine patches) and to date, the one most widely used is the lidocaine patch 5% which, according to Bianchi et al,77 would produce a complete response to treatment in 63% of HZ cases and 21% of PHN cases and if employed early would be able to prevent PHN. Überall et al,78 reported that in patients with PHN for more than a year, treatment for six months with “Lidocaine 700 mg medical plaster” had produced a significant reduction in pain, and in another even more recent study,79 it is stated that (based on the hypothesis of “ectopic pacemakers”)23 it even represents “a new breakthrough in the therapy of PHN”: further confirmation of the efficacy of this presidium comes from Giaccari et al.80 Finally, recommended by Yong et al,81 treatment with capsaicin 8% would be effective “in a trigeminal PHN of the I branch” started 2 months ago.10
The therapeutic rationale for subcutaneous steroid administration is to implement systemic anti-inflammatory treatment. For the subcutaneous administration of lidocaine, the therapeutic rationale is to temporarily silence the hyperexcitable nociceptors (considered the site of “ectopic pacemakers” in nociceptor hyperexcitability PHN) and with transdermal administration that of silencing them for as long as possible; in either case to reduce central hyperexcitability. Finally, capsaicin (like lidocaine and medicated patches) could also result in a kind of prolonged silencing of nociceptors in nociceptor hyperexcitability PHN.
Intrathecal methylprednisolone
To be carefully considered is the study by Kotani et al,75 re-presented a year later by Kirchner 82 where in 270 patients who had had PHN for at least one year an excellent-good outcome was reported in 90% of 89 patients who received intrathecal administration of 60 mg methylpredinosolone and 3 ml lidocaine 3% injected L2/L3 four times a week apart (taking advantage of trendelenburg to push the injected solution higher when needed), in 15% of 91 patients who received administration of lidocaine only, and in 5% of the 90 patients in the control group.
Rather puzzling and, in my opinion, also somewhat “pathetic” is a study 83 that included a small group of 10 patients and repeated the protocol of Kotani et al 75 comparing repeated administration 4 times 7 days apart of 60 mg of methylprednisolone acetate and intrathecal lidocaine with administration of lidocaine alone. This study found that the 6 patients who received methylprednisolone treatment had had increased pain at 8 weeks!
It is interesting to mention that Kotani et al 75 measured the concentration of interleukin-8 in CSF and found that it was markedly increased in patients with PHN, that the increase was inversely proportional to the duration of PHN, and that the concentration decreased in parallel with the reduction in pain after intrathecal methylprednisolone administration. The authors also observed that intrathecal methylprednisolone had been ineffective in 7 patients with PHN for more than 5 years because it was unlikely that a major inflammatory state was still present after such a long period and that therefore the inflammatory process was no longer at issue but nerve damage that could not be modified by treatment.
Ultimately, intrathecal administration of methylprednisolone may be effective as long as inflammation is present. Thus, the indication only covers PHN of types I and II.
Peridural block-infiltration and gasser's ganglion block-infiltration
Given that intrathecal use of methylprednisolone in a slow-release preparation is not recommended because of the risk of arachnoiditis (reported in exceptional cases anyway), perhaps the same result can be achieved with peridural administration.
As we have seen, peridural infiltration of steroids has been widely considered for prevention of PHN but only occasionally (and with reference to numerically limited case reports when not case reports) as a procedure to treat PHN, and with regard to Gasser's ganglion blockade-infiltration, the only reference is Pernak and Erdmann 40 which concerns prevention and not treatment of PHN.
In the experience of Shaker et al,84 in a PHN at C5 level had been present for 2 weeks (which may still have been HZ), transforaminal steroid infiltration resolved pain (in this case, however, rather than treatment perhaps it was prevention of PHN). In the experience of Mehta et al,85 a patient with PHN at T10 healed with transforaminal steroid infiltration. In the experience of Dinh et al,86 a patient with thoracic PHN healed after 3 transforaminal steroid infiltrations. Assessing the outcome of peridural steroid administration in 42 patients with HZ, Ghanavatian et al, 87 found that those with PHN for less than 11 months had a good outcome and not those who had it for longer. In the experience of Beydoun et al,3 with peridural infiltration of steroids and local anesthetics performed 1 to 3 times, in 20 patients (14 patients with pain for <3 months and 6 with PHN i.e., pain for >3 months), there was at 6 months after treatment a reduction in VAS from 8.3 to 1.8 in patients in the first group and from 7.8 to 4.3 in those in the second group.
Supporting the thesis of the inflammatory pathogenesis of PHN, in a study 88 included 44 patients presumably beyond the acute phase of HZ with symptoms from 30 to 180 days and thus likely with PHN in a phase still subject to remission, 21 patients (Group A) underwent a single peridural block with 5 mg dexamethasone, and 21 patients (Group B) after peridural catheter implantation left in place for 10 days were given 3 boluses of 5 mg dexamethasone (on days 1, 5, and 10) along with continuous infusion of Ropivacaine throughout. There was complete remission of pain in 28% of cases in Group A and 80% in Group B.
Referring back to the same pathogenetic assumption, perhaps the same result can be obtained as with intrathecal methylpredisolone by choosing the peridural steroid route but of this opinion were not Kikuchi et al 88 having found a markedly superior result in patients treated intrathecally with the protocol of Kotani et al.75
In any case, given the possible persistence of inflammation (perhaps only in types I and II PHN), it is worthwhile in any case to perform targeted antiphlogistic treatment with segmental peridural or Gasser's ganglion infiltration in the first 6 months after the onset of the disease: in the first 15 days to prevent PHN by taking advantage of sympathetic blockade, targeted antiphlogistic treatment, and (perhaps) blocking axonal transport of virus, and afterwards to treat it by eliminating the inflammatory portion that may still be present.
Treatment protocol (same as that proposed for treatment-prevention of PHN)
Segmental peridural block-infiltration with 2 ml of methylprednisolone (80 mg) and 5 ml of 0.5% bupivacaine to “wet” target root and those immediately above and below it, repeated after 2 weeks.
Block-infiltration of Gasser's ganglion with 1 milliliter of methylpredisolone (40 milligrams) and 2 milliliters of local anesthetic (bupivacaine 0.5%), according to the scheme proposed by Pernak and Erdmann 40 modified for the addition of buivacaine.
Pulsed radiofrequency (PRF) treatment of DRG and Gasser's ganglion
PHN in spinal nerves
A study 17 reports the results of Pulsed RF Treatment of DRG in a group of 29 patients with HZ-PHN for 3 months and in another group of 29 patients with PHN for 3-6 months: in the first group there was a good result in a greater percentage of subjects (...perhaps because having pain for less than 3 months they were more likely to recover spontaneously).
According to one observation, pulsed RF treatment of DRG associated with gapapentin would be more effective than gabapentin alone 89 because it would increase T-cell-mediated immunity and “inhibit the inflammatory response”. Treated 25 patients with PHN of upper extremity Ding et al,90 found a mean reduction of VAS from 7.5 to 2.5-3 that was established within one month and was still present at one year. To emphasize the efficacy of pulsed RF treatment on the DRG or intercostal nerve in patients with PHN, Huang91 states generically that and at 3 months after treatment, VAS was “significantly improved”. Finally, the efficacy of high-frequency pulsed RF is reported in a recent study where it is stated that it would reduce the number of Nav1.7 sodium channels in the DRG.92
Trigeminal PHN
Treated 45 patients with trigeminal PHN Ding et al,93 found a mean reduction of VAS from 6.5 to 2.5 that became progressively established within 1 month and was still present at 1 year. Liu et al94 subjected 32 patients with PPH of the I trigeminal branch present from 6 months to 3 years to Gasser's ganglion Pulsed RF Treatment: 30/32 patients achieved a marked reduction of pain (VAS 0-3) from the first week and at a 3-month follow-up. Regardless of the type of PHN that has not been elucidated, overall the results seem satisfactory: improvements from spontaneous healing are unlikely considering that patients had PHN from 6 months to 3 years. Li et al 8 affirm a reduction in trigeminal PHN pain in the I branch at 1-3-6 months after the procedure with pulsed RF treatment of supraorbital nerve, pointing out that high-voltage pulsed RF is more effective than conventional RF. Pulsed RF of Gasser's ganglion is recommended by Wan et al 95 who performed it in patients with trigeminal PHN for less than 3 months, describing it as being in the “acute-subacute phase”: in fact, spontaneous healing is still possible in them. Finally, although it is unclear under what criteria trigeminal and upper extremity PHN are associated, some results would have been obtained in facial and upper extremity PHN with stellate ganglion blockade and...pulsed RF treatment of the stellate ganglion.93
Pulsed RP would increase the C-fos gene in nerve cells of DRG and in dorsal horn of the spinal cord, which in turn would increase the activity of inhibitory interneurons. In support of this reasoning, it was observed that ¼ of the spinal neurons expressing the C-fos gene are inhibitory interneurons (glycinergic, GABA-ergic 96 and dynorphinergic) whose increase corresponds to the activation of the antinociceptive mechanism known as “long term depression”.97
Advancing doubts about the neuromodulation thesis, Erdine et al 98 studied by electron microscopy the DRG of rat treated with pulsed RF current and found cellular damage consisting of degeneration of mitochondria, enlargement of endoplasmic reticulum cisternae, and loss of nuclear membrane, concluding that pulsed RF current is “less neurolesive” than continuous RF current but is not a nondestructive technique. Corollary to these findings, Protasoni et al 99 found nerve damage limited to myelin sheaths.Supporting hypothesis that pulsed RF applied on the DRG or Gasser's ganglion activates an inhibitory mechanism, one has to ask what it acts on and thus in what kind of PHN.
Reconsidering the work of Liu et al 94 on Pulsed RF Treatment of Gasser's ganglion, we note that they performed the delivery of pulsed RF current for 8 minutes by programming it to limit the temperature of the tissue around the electrode to 42°C, with an impedance of 200-300 Oms and an electrode with an active tip of 2 mm thus in a position on the borderline between the trigeminal cisterna (where impedance is 200 Oms) and Gasser's ganglion (where impedance that is detected is 400 Oms). Technically, one should place the active tip of the electrode in the compagine of Gasser's ganglion (so a 2-mm active tip electrode may be appropriate) but the impedance should be definitely above 300 Oms: in practice, the advisable procedure should be to reach the trigeminal cistern (verifying CSF leakage and an impedance of 200 Oms) and then withdraw the electrode until its tip is placed in the ganglion compagine, verifying the cessation of CSF aspiration and the impedance rising to 400 Oms.
Another consideration should be made about the observations of Han et al,100 who conducted a study of 109 patients with thoracic PHN and employed “high voltage” pulsed RF (65 V) claiming that it is more likely to be effective...but occasionally produces mild numbness of the skin (partial neurolesion effect?). Of the same opinion were Wan et al 95 confirming the greater efficacy of high-voltage pulsed RF over standard RF. On the other hand, in support of the neuromodulation thesis, the importance of the electric field produced by pulsed RF current was emphasized. Although the continuous one also produces an electric field, the one produced by the pulsed RF current would be “stronger” perhaps because the shortness of the voltage peaks allows the use of a higher voltage.
Indications of pulsed RF treatment of DRG and Gasser's ganglion
Accepting the hypothesis that pulsed RF applied on the DRG or Gasser's ganglion activates an inhibitory mechanism, it is useful when there is an afferent to be inhibited and thus in nociceptor hyperexcitability PHN where it would inhibit excess activity in C fibers. Debatable is its indication in demyelination PHN where it should inhibit Aδ fibers and in axonal neuropathy PHN where it should inhibit Aβ. Certainly it cannot act in deafferentation PHN where there is nothing to inhibit nor in central PHN.
Thus, Pulsed RF Treatment of the DRG and Gasser's ganglion is indicated only in nociceptor hyperexcitability PHN and, producing a partial and transient result with a high probability of recurrence, is of limited usefulness and also implies periodic repetition of the procedure...perhaps while waiting for the hoped-for spontaneous healing.Spinal Cord Stinulation (SCS)
The mechanism of action of SCS is classically considered to be the activation of Aβ inhibitory afferents, and lead implantation techniques have been developed on these premises. In recent years, however, attention toward SCS has shifted to two major technological innovations that have called into question the mechanisms of action and given new hope: these are “High Frequency SCS” introduced in 2010 and “Burst SCS” introduced in 2013.
There are not many experiences about SCS in the treatment of PHN. In that of Meglio et al,101 10 patients underwent to temporary implantation to test the efficacy of SCS: 6/10 had >50% reduction in pain intensity and underwent definitive implantation with a favorable outcome that continued at a follow-up of 15-46 months, and in that of Baek et al,102 11 patients underwent the test but only 4 then underwent definitive implantation with a favorable antalgic outcome (VAS less than 3) that continued during a follow-up of 2 years.
The efficacy of SCS was supported by Iseki et al 103 and Moriyama 104 and in a recent review of literature 105 including 243 patients it appears that it produced a mean reduction in VAS from 7.6 to 2.7 at an 18-month follow-up. Recently, Liu 94 recommended short-term spinal cord electrical stimulation and others supported the efficacy of SCS and spinal nerve electrostimulation.106
More than 40 years ago, Larson et al 107,108 questioned the mechanism of action of SCS centered on the activation of large myelin afferents, reporting the efficacy of electrostimulation of the anterior half of the cord and hypothesized that responsible for pain relief from SCS was not activation of posterior chordae but conduction blockade of spinothalamic pathways. Along the same line of thought, implanted electrodes in the subarachnoid space at the C1-C2 level, Hoppenstein 109,110 obtained pain relief with a current of 30 times lower intensity when the electrodes were placed in front of the lateral spinothalamic bundle than when they were placed posteriorly and observed that in the former case pain relief was contralateral to the stimulated site. To confirm these observations, note that often during Cordotomy, patient reports the temporary disappearance of contralateral pain even before lesion, when the electrode has penetrated the lateral spinothalamic bundle and sensory electrostimulation is performed. In those same years, Campbell and Taub 111 and Ignelzi and Nyquist 112 formalized the hypothesis that neurostimulation, instead of “adding impulses to nerve”, would “reduce the number of impulses”, resulting in “conduction blockade”. In turn, conduction block would be due to accumulation of K ions around the axon and the consequent reduction in conductance of Na channels. In practice, the current that stimulates the nerve would collide with the electrical stimulus that runs orthodromically through the nerve fibers, blocking it (collision current theory).113,114
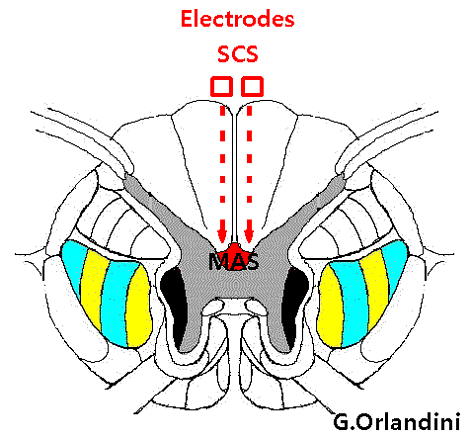
If the conduction block hypothesis is accepted, it is obvious that the target to be stimulated shifts from large myelin afferents to small fibers Ad and C, and the implantation technique and stimulation parameters change. In fact, conduction block does not affect the ascending fibers of spinal lemniscus, which are quite distant from the site where the electrode is placed, with interposition of the pyramidal bundle: instead, multisynaptic ascending system (MAS) fibers are relatively close to the electrode and are likely to be the ones involved by the high-frequency SCS and “Burst SCS” (Figure 5). Given that it is MAS that is responsible for the conduction of TAP originating from the second neuron in neuropathic pain, this mechanism would explain the effect of HT-SCS and Burst-SCS on neuropathic pain and would also explain why “classical” SCS was not as effective.
{kind=link}
Indications of the SCS in the PHN
Reconsidering the meagre data in the literature, it appears that some patients responded favorably to SCS and others did not: likely the positive or negative outcome depended on the type (which is not mentioned) of PHN. In conclusion, SCS might be indicated in axonal neuropathy PHN and demyelination PHN, is useless in central PHN that does not depend on MAS and superfluous in nociceptor hyperexcitability PHN. As for the usefulness of SCS in deafferentation PHN, if it really acts on MAS, its efficacy cannot be ruled out (Figure 6).
{kind=link}
DREZ-lesion
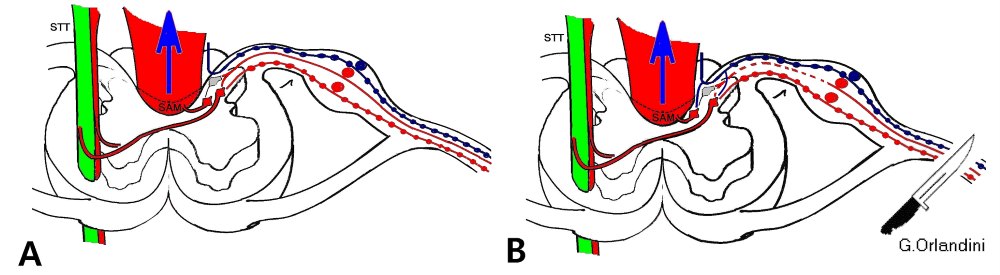
Dorsal Root Entry Zone lesion (DREZ-lesion) is radiofrequency thermolesion of the first 5-6 laminae of Rexed that constitute the dorsal root entry zone (DREZ) and contain the second neurons from which the central nociceptive pathways originate (Figure 7). The operation is performed with an open technique and with the support of operating microscope.
The results obtained by Friedman, Nashold and Ovelmen-Levitt 115 in the treatment of PHN are encouraging: out of 12 patients treated, 6 achieved complete and persistent pain relief, and a more recent review of the literature 116 including 84 patients with PHN present with a mean of 3.6 years, shows that DREZ lesion produced a mean reduction in VAS from 8.7 to 3.7 at a 10-year follow-up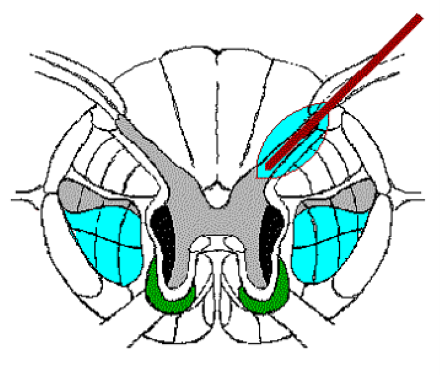{kind=link}
DREZ-lesion 117-120 exerts its antalgic effect by disrupting pain generating mechanisms 121 in the dorsal horn of spinal cord and particularly the cells of origin of paleospinothalamic pathways. Indeed, it appears that the electrical activity underlying neuropathic pain is conducted by central afferents different from those that conduct normal tissue pain nociception, namely by MAS rather than lemniscal pathways (Figure 6). This difference would depend on the fact that MAS-derived cells are tonically inhibited by nociceptive afferents and when these decrease as they do in neuropathic pain their activity increases.121
Indications of DREZ-lesion
Limited to spinal nerve-loaded PHN, DREZ-lesion might be indicated in the deafferentation PHN and axonal-demielination neuropathy PHN while it is unnecessary in the central non-MAS-dependent PHN and superfluous in nociceptor hyperexcitability PHN.
Trigeminal nucleotomy is lesion of the junctional zone between the first and second trigeminal neurons in the caudal subnucleus. This structure, called the “medullary dorsal horn”, 122 is the cranial continuation of dorsal horn of the spinal cord and is anatomo-functionally the homologue of spinal DREZ. It follows from this that trigeminal nucleotomy is the homologue of spinal DREZ-lesion and as such, has been proposed to treat “deafferentation facial pain”.123,124 Trigeminal nucleotomy can be performed with the stereotactic posterior technique , with the percutaneous posterolateral technique or with the “percutaneous lateral technique” that I have perfected and that, to the best of my knowledge, only I have performed.125 Unfortunately, since the caudal subnucleus is not a bundle of fibers but an agglomeration of cells, it can only be destroyed by a lesion that is sufficiently extended longitudinally to encompass most of it. This involves a series of lesions with repositioning of the electrode along the longitudinal plane, and lesion is painful because the tip of electrode directed so obliquely is in a subpial position. This technique would deserve to be perfected but in the age of award-winning mediocrity certainly one prefers to rely on “medicated patches”…
Subarachnoid drug therapy
After implantation of intrathecal catheter connected to infusion pump, midazolam and opioids were administered. According to a review of the literature,106 patients given midazolam had >50% pain reduction and those given opioids had 41% pain reduction: in half of the cases, treatment was discontinued due to side effects and loss of efficacy. Recently, administration of morphine or hydromorphone peridurally after placement of catheter placed with the tip at the metamerus affected by PHN at a rate of 1ml/h for 72 hours has been proposed 126 and (if one is willing to believe it) it was claimed that the antalgic effect lasted for two weeks after treatment.
Rationalization of PHN therapy
Remembering that in PHN there is an association of multiple pathogenetic types, it is necessary to identify them and recognize the predominant one. Given this, from the point of view of therapy, a suggestion that applies to all types of PHN initiated no more than 6 months ago (trusting that a pathogenetically relevant inflammatory process may still be in progress), is to proceed with peridural or Gasser's ganglion block-infiltration repeated after 2 weeks to prevent aggravation of nerve damage.
Because of important procedural differences, it is convenient to consider spinal nerve PHN therapy and trigeminal nerve therapy separately.
Therapy of persistent nociceptor hyperexcitability PHN
In this type of PHN, often destined to recover quickly, subcutaneous infiltration of local anesthetics and steroids, medicated patches, capsaicin, NSAIDs and minor opioids (tramadol and tapentadol) may be sufficient. If these treatments do not have the desired effect, pulsed radiofrequency treatment (RFP) of the DRG or Gasser's ganglion may be considered to inhibit excess activity in the C-fibers possibly repeated periodically if, as is to be expected, the result is temporary.
Therapy of axonal neuropathy PHN
In axonal neuropathy PHN, amitriptyline (75 mg/day) employed to exploit its effect of potentiating the serotonergic descending inhibitory pathway of DLF and, alternatively, duloxetine (60 mg/day) is effective. If these treatments do not have the desired effect, HT-SCS or Burst-SCS may be considered for their action of blocking conduction in MAS, which is involved in the conduction of TAP originating from the second neuron in neuropathic pain. In the case of axonal neuropathy PHN in the trigeminal region, unfortunately, no similar resources are available and only the extreme remedies considered for desperate cases remain.
Therapy of demyelination PHN
In demyelination PHN, carbamazepine, oxacarbazepine, or lamotrigine are effective. If these treatments do not have the desired effect, HT-SCS or Burst-SCS may be considered for their action of blocking conduction in the MAS which is involved in the conduction of the TAP originating from the second neuron in neuropathic pain and in the case of demyelination PHN at the trigeminal level RF Trigeminal Thermorhizotomy with the aim of producing a lesion at the Aδ fibers as is done to treat Trigeminal Neuralgia in Multiple Sclerosis.
Therapy of deafferentation PHN
NPH affecting spinal nerves
In deafferentation PHN, with the goal of blocking calcium channels in the second neuron to limit its spontaneous activation, high-dose gabapentin (1600 mg/day) and/or baclofen 75 mg/day (also in combination) may be useful. If these treatments do not have the desired effect, one can only hope on: 1) DREZ-lesion; 2) HT-SCS or Burst-SCS (potentially effective if one admits that they act by blocking conduction in the MAS which is involved in TAP conduction in neuropathic pain including deafferentation pain.
PHN affecting trigeminal nerve
Bearing in mind that deafferentation PHN is a very serious problem here, with the goal of blocking calcium channels in the second neuron to limit their spontaneous activation, high-dose gabapentin (1600 mg/day) and/or baclofen 75 mg/day (also in combination) may be useful. If these treatments do not have the desired effect, one might consider trigeminal nucleotomy...if someone were able to perform it! Outside of this procedure, there are unfortunately no other resources available and only the extreme remedies considered for desperate cases remain.
Treatment of desperate cases
In really serious and intractable cases that are otherwise intractable, it is permissible to consider aggressive solutions with pharmacological treatments directed at inducing a kind of psychological dissociation that interferes with the production of the pain emotion: neuroleptic drugs and in extreme cases psychosurgery are available for this purpose.
Among neuroleptics, fluphenazine 127 haloperidol 128,129 and especially chlorpromazine 130,131 may be useful. Chlorpromazine (Largactil cp 25-100 mg, administered at 1/8 hr dose) might be particularly interesting because, according to one report (actually the only one I could find) it would block Nav1.7 sodium channels resulting in elevation of pain perception threshold.132
As for the extreme remedy of psychosurgery, remember that it consists in the interruption of the thalamus-fronto-limbic connections and is directed at the suppression of the mechanisms that affectively interpret somatosensory stimuli, including nociception. Theoretically, with psychosurgical operations, the control of suffering is achieved without analgesia and therefore nociceptive stimuli are still felt and recognised after these operations, but pain no longer disturbs, since an indifference to pain has been achieved that used to lead to severe psychological and intellectual deterioration with classic prefrontal lobotomy (or leukotomy). Fortunately, today, with modern cingulotomy, such deficits are more nuanced and inconstant.
Conflict of interests
The authors declares no conflict of interests
Open Access-license (CC BY-NC 4.0)
Published
30th June 2024
Bibliografia
2. Zhang Z. et al. Analysis of Efficacy and Factors Associated with Recurrence After Radiofrequency Thermocoagulation in Patients with Postherpetic Neuralgia: a Long-Term Retrospective and Clinical Follow-Up Study. Pain Ther., 11 (2022) 971-985
4. Thompson RR. et al. Herpes Zoster and Postherpetic Neuralgia: Changing Incidence Rates From 1994 to 2018 in the United States. Clin Infect Dis., 73 (2021) e3210-e3217.
5. Ngo L. et al. Postherpetic Neuralgia: Current Evidence on the Topical Film-Forming Spray with Bupivacaine Hydrochloride and a Review of Available Treatment Strategies. Adv Ther., 37 (2016) 2003-2016
6. Follini L. Herpes zoster e prevenzione della nevralgia post-herpetica. Esperienza e valutazione dei risultati di 10 anni di attività del Centro di Terapia del Dolore di Parma. Int.Journal of Pain Therapy, 3 (1993) 154-159
7. Paisley P., Serpell N. Diagnosis and management of postherpetic neuralgia. Practitioner, 259 (2015) 21-4
8. Li H. et al. Effective Treatment of Postherpetic Neuralgia at the First Branch of the Trigeminal Nerve by High-Voltage Pulsed Radiofrequency. Front Neurol., 12 (2021) 746035
9. Gilden G. Efficacy of live zoster vaccine in preventing zoster and postherpetic nevralgia. J Intern Med., 269 (2011) 496-506.
10. Lipton S. Post-herpetic neuralgia. In Lipton S. (Ed.). Relief of pain in clinical practice. Blackwell Scientific Publications, Oxford-London-Edinburgh-Melbourne 1979, pp.231-248
11. Warren-Gash C., Harriet Forbes H. , Judith Breuer J. Varicella and herpes zoster vaccine development: lessons learned Expert Rev Vaccines, 16 (2017) 1191-1201
12. Noordenbos W. Pain. Elsevier, Amsterdam 1959
13. Melzack R. and Wall P.D. Pain mechanisms: a new theory. Science, 150 (1965) 971-978
14. Schon F., Mayer M.L., Kelly J.S. Pathogenesis of post‑herpetic neuralgia. The Lancet, August 15 (1987) 366‑368
15. Watson C.P.N., Deck J.H., Morshead C., Van Der Kooy D. and Evans R.J. Post‑herpetic neuralgia: further post-mortem studies of cases with and without pain. Pain, 44 (1991) 105-117.
16. Devor M. Rethinking the causes of pain in herpes zoster and postherpetic neuralgia: the ectopic pacemaker hypothesis. 3 (2018) e702
17. Kim J.Y. et al. Usefulness of Inflammatory Markers for the Prediction of Postherpetic Neuralgia in Patients with Acute Herpes Zoster. Ann Dermatol., 30 (2018) 158-163.
18. Mashhood A. The efficacy of local infiltration of triamcinolone acetonide with lignocaine compared with lignocaine alone in the treatment of postherpetic nevralgia. J Coll Physicians Surg Pak, 15 (2005) 683-5.
18. Mashhood A. The efficacy of local infiltration of triamcinolone acetonide with lignocaine compared with lignocaine alone in the treatment of postherpetic nevralgia. J Coll Physicians Surg Pak, 15 (2005) 683-5.
19. Colding A. The effect of regional sympathetic blocks in the treatment of herpes zoster. Acta Anaesthesiol. Scand., 13 (1969) 133-141
20. Leriche R. La chirurgie de la douleur. Masson, Paris 1939
21 Livingston W.K. Pain mechanisms: a physiologic interpretation of causalgia and its related states. Macmillan, London 1944
22. Winnie A.P., Hartwell P.W. Relationship between time of treatment of acute herpes zoster with sympathetic blockade and prevention of post-herpetic neuralgia: clinical support for a new theory of the mechanism by wich sympathetic blockade provides therapeutic benefit. Reg.Anesth., 18 (1993) 277-282
23. Peng W.W. et al. Biological mechanism of post-herpetic neuralgia: Evidence from multiple patho-psychophysiological measures. Eur J Pain, 21 (2017) 827-84218. Calvin W.H., Loeser J.D., Howe J.F. A neurophysiological theory for pain mechanism of tic douloureux. Pain, 3 (1977) 147‑154
24. Robinson D.M., Perry C.M. Zoster vaccine live (Oka/Merck) Drugs Aging, 23 (2006) 525-31
25. Arnold N., Messaoudi I. Herpes zoster and the search for an effective vaccine. Clin Exp Immunol., 187 (2017) 82-92
26. Singh G. et al. Recombinant zoster vaccine (Shingrix®): a new option for the prevention of herpes zoster and postherpetic neuralgia. Korean J Pain, 33 (2020) 201-20727. Oxman M.N. et al., Shingles Prevention Study Group A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med, 35 (2005) 2271-84
28. Klein N.P. et al. Long-term effectiveness of zoster vaccine live for postherpetic neuralgia prevention. Vaccine, 37 (2019) 5422-5427
29. Cunningham A.L. et al. Efficacy of the Herpes Zoster Subunit Vaccine in Adults 70 Years of Age or Older N Engl J Med, 357 (2016) 1019-32
30. Izurieta H.S., Wu X., Forshee R., Yun Lu R., Sung H.M., Agger P.E., Chillarige Y., Link-Gelles R., Lufkin B., Wernecke M., MaCurdy T.E., Kelman J., Dooling K. Recombinant Zoster Vaccine (Shingrix): Real-World Effectiveness in the First 2 Years Post-Licensure. Clin Infect Dis., 73 (2021) 941-948.
31. Mbinta J.F. et al. Post-licensure zoster vaccine effectiveness against herpes zoster and postherpetic neuralgia in older adults: a systematic review and meta-analysis. Lancet Healthy Longev., 3 (2022) e263-e275.
32. Herbort C.P. et al. High-dose oral acyclovir in acute herpes zoster ophthalmicus: the end of the corticosteroid era. Curr Eye Res., 10 (1991) 171-5.
28. Klein N.P. et al. Long-term effectiveness of zoster vaccine live for postherpetic neuralgia prevention. Vaccine, 37 (2019) 5422-5427
29. Cunningham A.L. et al. Efficacy of the Herpes Zoster Subunit Vaccine in Adults 70 Years of Age or Older N Engl J Med, 357 (2016) 1019-32
30. Izurieta H.S., Wu X., Forshee R., Yun Lu R., Sung H.M., Agger P.E., Chillarige Y., Link-Gelles R., Lufkin B., Wernecke M., MaCurdy T.E., Kelman J., Dooling K. Recombinant Zoster Vaccine (Shingrix): Real-World Effectiveness in the First 2 Years Post-Licensure. Clin Infect Dis., 73 (2021) 941-948.
31. Mbinta J.F. et al. Post-licensure zoster vaccine effectiveness against herpes zoster and postherpetic neuralgia in older adults: a systematic review and meta-analysis. Lancet Healthy Longev., 3 (2022) e263-e275.
32. Herbort C.P. et al. High-dose oral acyclovir in acute herpes zoster ophthalmicus: the end of the corticosteroid era. Curr Eye Res., 10 (1991) 171-5.
33. Chen L. et al. Efficacy and safety of the extracorporeal shockwave therapy in patients with postherpetic neuralgia: study protocol of a randomized controlled trial. Trias, 21 (2020) 630.
34. Bauman J. Treatment of acute herpes zoster neuralgia by epidural or stellate ganglion block. Anesthesiology, Suppl.51 (1979) S223.
35 Dan K., Higa K. and Noda B. Nerve block for herpetic pain. In Fields H.L. et Al.(Eds.). Advance in pain research and therapy. Vol.9. Raven Press, New York 1985, pp.831-838
36. Tenicela R., Lovasik D. and Eaglstein W. Treatment of herpes zoster with sympathetic blocks. Clin. J. Pain, 1 (1985) 64
37. Winnie A.P. The treatment of acute herpes zoster and prevention of post-herpetic neuralgia by sympathetic blockade: rationale and results. 6th International Congress: Pain Clinic, April 15-20, 1994, pp.226-229
38 Wu C.L., Massh A., Dworkin R.H. The role of sympathetic nerve blocks in herpes zoster and postherpetic neuralgia. Pain, 87 (2000) 121-129
39. Yanagida H, Suwa K, Corssen G. No prophylactic effect of early sympathetic blockade on postherpetic neuralgia. Anesthesiology 66 (1987) 73‑76
40. Pernak J, Erdmann W. Acute herpes zoster of trigeminal nerve and its treatment. 6th International Congress: Pain Clinic, April 15-20, 1994, pp.221-225
41 Orlandini G. La decisione terapeutica nella medicina del dolore: dalla diagnosi patogenetica alla scelta motivata della terapia. Delfino Ed., Roma 2020
42 Perkins H.M., Hanlon P.R. Epidural injection of local anesthetic and steroids for relief of pain secondary to herpes zoster. Arch. Surg., 113 (1978) 253-254
43. Follini L., Leccabue M. Prevention of post-herpetic neuralgia. Personal resulsts of ten years’ experience. Proceedings of the 6th International Congress of Pain Clinic, Atlanta-Georgia, USA, April 15-20, 1994
44. Hwang et al. The effects ofepidural blockade on the acute pain in herpes zoster. Arch.Dermatol., 135 (1999) 1359-1354
45. Pasqualucci A., Pasqualucci V., Galla F., DeAngelis V., Marzocchi V., Colussi R., Paletti F., Girardis M, Lugano M. and DelSindaco F. Prevention of post-herpetic neuralgia: acyclovir and prednisolone versus epidural local anesthetic and methylprednisolone. Acta Anaesthesiol.Scand., 44 (2000) 910-918
46. Kumar V. et al. Neuraxial and sympathetic blocks in herpes zoster and postherpetic nevralgia: an appraisal of current evidence. Reg.Anesth.Pain Med., 20 (2004) 454-461
47. Opstelten W., VanWijck A.J., VanEssen G.A., Buskens E., Bak A.A., Kalkman C.J., Verheij T.J.M., Moons K.G.M. The PINE study: rationale and design of a randomised comparison of epidural injection of local anaesthetics and steroids versus care-as-usual to prevent postherpetic neuralgia in the elderly. BMC Anesthesiol., 4 (2004) 2
48. Opstelten W., VanWijck A.J., VanEssen G.A., Moons K.G.M., Verheij T.J.M., Kalkman C.J., Von Hout B.A. Cost effectiveness of epidural injection of steroids and local anesthetics for relief of zoster-associated pain. Anesthesiology, 107 (2007) 678-679
49. Opstelten W., VanWijck, Moons K.G.M., VanEssen G.A., Stolker R.J., Kalkman C.J., Verheij T.J.M. Treatment of patients with herpes zoster by epidural injection of steroids and local anaesthetics: less pain after 1 month, but no effect on long-term postherpetic neuralgia--a randomised trial. Ned Tijdschr Geneeskd., 150 (2006) 2649-55
50. VanWijck A.J.M., Opstelten W., Moons K.G.M., VanEssen G.A., Stolker R.J., Kalkman C.J., Verheij T.J.M. The PINE study of epidural steroids and local anaesthetics to prevent postherpetic neuralgia: a randomised controlled trial. Lancet, 367 (2006) 219-24
51. Loeser J.D. Herpes zoster and postherpetic neuralgia. In Bonica J.J.et Al (Eds.). The management of pain. Lea & Febiger, Philadelphia, London 1990, pp.257-263
52. Kim J.Y. et al. Usefulness of Inflammatory Markers for the Prediction of Postherpetic Neuralgia in Patients with Acute Herpes Zoster. Ann Dermatol., 30 (2018) 158-163
53. Gross E. et al. S2k guidelines for the diagnosis and treatment of herpes zoster and postherpetic neuralgia. J Dtsch Dermatol Ges., 18 (2020) 55-78
54. Lavoie P.A. et al. Block of fast axonal transport in vitro by the local anesthetics dibucaine and etidocaine. J Pharmacol Exp Ther., 223 (1982) 251-6
55. Lavoie P.A. Inhibition of fast axonal transport in vitro by the local anesthetics prilocaine, mepivacaine, and bupivacaine. Can J Physiol Pharmacol., 61 (1983) 1478-82
56. Lavoie P.A. et al. Mechanisms of the inhibition of fast axonal transport by local anesthetics. Neuropharmacology, 28 (1989) 175-81
57. Aggarwal A. et al. Post-herpetic Neuralgia: A Systematic Review of Current Interventional Pain Management Strategies. J Cutan Aesthet Surg., 13 (2020) 265-274
58. Thomas B., Farquhar-Smith P. Extended-release gabapentin in post-herpetic neuralgia. Expert Opin Pharmacother., 12 (2011) 2565-71
59. Gan E.Y. et al. Management of herpes zoster and post-herpetic neuralgia. Am J Clin Dermatol. 14 (2013) 77-85
60. Hadley G.R., Gayle J.A., Ripoll J., Jones M.R., Argoff C.E., Kaye R.J., Kaye A.D. Post-herpetic Neuralgia: a Review. Curr Pain Headache Rep., 20 (2016) 17
61. Saguil A. et al. Herpes Zoster and Postherpetic Neuralgia: Prevention and Management. Am Fam Physician, 96 (2017) 656-663
62. Shrestha M., Chen A. Modalities in managing postherpetic nevralgia. Korean J Pain, 31 (2018) 235-243
63. Cao X. et al. A Meta-analysis of Randomized Controlled Trials Comparing the Efficacy and Safety of Pregabalin and Gabapentin in the Treatment of Postherpetic Neuralgia. Pain Ther., (2022)
64. Kawai S. et al. Efficacy and safety of twice-daily tramadol hydrochloride bilayer sustained-release tablets with an immediate release component for postherpetic neuralgia: Results of a Phase III, randomized, double-blind, placebo-controlled, treatment-withdrawal study. Pain Pract., (2022)
65. Wen B. et al. Efficacy of different interventions for the treatment of postherpetic neuralgia: a Bayesian network meta-analysis. J Int Med Res., 48 (2020)
66. Lin C.-S. et al. Interventional Treatments for Postherpetic Neuralgia: A Systematic Review. Pain Physician, 22 (2019) 209-228
67. Fields H.L., Rowbotham M., Baron R. Postherpetic neuralgia: irritable nociceptors and deafferentation. Neurobiol Dis., 5 (1998) 209-27
68. Forstenpointner J. et al. Up-date on Clinical Management of Postherpetic Neuralgia and Mechanism-Based Treatment: New Options in Therapy. J Infect Dis., 218 (2018) S120-S126
69. Epstein E. Treatment of zoster and postzoster neuralgia by the intralesional injection of triamcinolone: a computer analysis of 199 cases. Int J Dermatol., 15 (1976) 762-9
70. Riopelle J.M., Naraghi M. and Grush K.P. Chronic neuralgia incidence following local anesthetic therapy for herpes zoster. Arch. Derm., 120 (1984) 747-750
xx
xx
71. Bhargava R., Bhargava S., Haldia K.N., Bhargava P. Jaipur block in postherpetic nevralgia. Int J Dermatol., 37 (1998) 465-8
72. Puri N. Modified Jaipur block for the treatment of post-herpetic nevralgia. Int J Dermatol,, 50 (2011) 1417-1420
73. Sharma R.K., Gupta M., Tegta G.R., Verma G., Rani R. Post Herpetic Neuralgia: A Retrospective Study to Evaluate Response to Modified Jaipur Block with Increased Concentration of Dexamethasone. Indian J Dermatol., 66 (2021) 459-464
74. Nguyen D.T. et al. The effect of subcutaneous injection of methylprednisolone acetate and lidocaine for refractory postherpetic neuralgia: a prospective, observational study Health Sci Rep., 4 (2021) e271
75. Kotani N. et al. Intrathecal methylprednisolone for intractable postherpetic nevralgia. N Engl J Med., 343 (2000) 1514-9
76 Liu X. et al. The Treatment of Topical Drugs for Postherpetic Neuralgia: A Network Meta-Analysis. Pain Physician, 23 (2020) 541-551
77. Bianchi L. et al. Effectiveness and safety of lidocaine patch 5% to treat herpes zoster acute neuralgia and to prevent postherpetic neuralgia. Dermatol Ther., 34 (2021) e14590
78. Überall M.A., Eerdekens M., Hollanders E., Bösl I., Sabatschus I. Lidocaine 700 mg medicated plaster for postherpetic neuralgia: real-world data from the German Pain e-Registry. Pain Manag., 12 (2021) 195-209
79. Fornasari D., Magni A., Pais P., Palao T., Polati E., Sansone P. Changing the paradigm in postherpetic neuralgia treatment: lidocaine 700 mg medicated plaster. Eur Rev Med Pharmacol Sci., 26 (2022) 3664-3676
80. Giaccari L.G., Ausilio C., Coppolino F., Pace M.C., Passivanti M.B., Pota V., Sansone P. Lidocaine 700 mg medicated plaster for post-herpetic neuralgia: focus on Quality of Life, effectiveness and safety - a retrospective observational study. Eur Rev Med Pharmacol Sci., 26 (2022) 130-137
81 Yong Y.L. et al. The Effectiveness and Safety of Topical Capsaicin in Postherpetic Neuralgia: A Systematic Review and Meta-analysis. Front Pharmacol., 10 (2017) 538
82 Kirchner J.T. Intrathecal Methylprednisolone for Postherpetic Nevralgia Am Fam Physician.63 (2001) 1883-1840
83. Rijsdijk M. et al. No beneficial effect of intrathecal methylprednisolone acetate in postherpetic neuralgia patients. Eur J Pain, 17 (2013) 714-23
84. Shaker A. et al. Postherpetic neuralgia involving the right C5 dermatome treated with a cervical transforaminal epidural steroid injection: a case report. Arch Phys Med Rehabil., 88 (2007) 255-8
85. Mehta P., Maher P., Singh J.R. Treatment of postherpetic neuralgia using a thoracic transforaminal epidural steroid injection. 7 (2015) 443-6
86. Dinh B.N et al. Serial Thoracic Transforaminal Epidural Steroid Injections for Post-herpetic Neuralgia: A Case Report. Cureus 14 (2022) e21808.
87. Ghanavatian S. et al. Parameters associated with efficacy of epidural steroid injections in the management of postherpetic neuralgia: the Mayo Clinic experience. J Pain Res., 12 (2019) 1279-1286
88. Kikuchi et al. Comparative yherapeutic evaluation on intrathecal versus epidural methylprednisolone fon long-term analgesia in patients with intractable postherpetic nevralgia. Reg.Anesth.Pain Med., 24 (1999) 287-293
89. Huang Y. et al. Clinical observations on selective dorsal root ganglion pulsed radiofrequency lesioning combined with gabapentin in the treatment of postherpetic neuralgia. Neurol India, 66 (2018) 1706-1710
90. Ding Y. et al. Efficacy of Pulsed Radiofrequency to Cervical Nerve Root for Postherpetic Neuralgia in Upper Extremity. Front Neurosi., 14 (2020) 377
91. Huang X. Efficacy and safety of pulsed radiofrequency modulation of thoracic dorsal root ganglion or intercostal nerve on postherpetic neuralgia in aged patients: a retrospective study. BMC Neurol., 21 (2021) 233
92. Ding Y. et al. Efficacy of CT Guided Pulsed Radiofrequency Treatment for Trigeminal Postherpetic Neuralgia. Front Neurosi., 13 (2019b) 708
93. Ding Y. et al. CT-Guided Stellate Ganglion Pulsed Radiofrequency Stimulation for Facial and Upper Limb Postherpetic Neuralgia. Front Neurosi., 13 (2019a) 170
94. Liu Q. et al. Analgesic Effect of Electroacupuncture on Postherpetic Neuralgia: A Trial Protocol for a Multicenter Randomized Controlled Trial. Pain Ther., 10 (2021) 1755-1771
95. Wan C.F., Song T. Comparison of Two Different Pulsed Radiofrequency Modes for Prevention of Postherpetic Neuralgia in Elderly Patients With Acute/Subacute Trigeminal Herpes Zoster. Neuromodulation, 25 (2022) 1364-1371.
96. Todd A.J., Spike R.C., Broadbelt A.R., Price R.F., Shehab S.A. Some inhibitory neurons in the spinal cord develop c-fosimmunoreactivity after noxious stimulation. Neurosciense, 63 (1994) 805-816
97. Sandkuhler J., Chen J.G., Cheng G. and Randic M. Low-frequency stimulation of afferent Aδ-fibers induces long-term depression at primary afferent synapses with substantia gelatinosa neurons in the rat. J.Neurosci., 17 (1997) 6483-6491
98. Erdine S., Yucel A., Cimen A., Aydin S., Sav A., Bilir A. Effect of pulsed versus conventional radiofrequency current on rabbit dorsal root ganglion morphology. European Journal of Pain, 9 (2005) 251-256
99. Protasoni M, Reguzzoni M, Sangiorgi S et al. Pulsed radiofrequency effects on the lumbar ganglion of the rat dorsal root: a morphological light and transmission electron microscopy study at acute stage. Eur Spine J., 18 (2009) 473-478
100. Han Z. et al. CT-Guided Pulsed Radiofrequency at Different Voltages in the Treatment of Postherpetic Neuralgia. Front Neurosi., 14 (2020) 579486
101. Meglio M., Cioni B., Prezioso S., Talamonti D. Spinal cord stimulation (SCS) in the treatment of postherpetic pain. Acta Neurochir Suppl (Wien), 46 (1989) 65-6
102. Baek I.Y. et al. Spinal cord stimulation in the treatment of postherpetic neuralgia in patients with chronic kidney disease: a case series and review of the literature. Korean J Pain, 24 (2011) 154-7
103. Iseki M. et al. Efficacy of limited-duration spinal cord stimulation for subacute postherpetic nevralgia. Ann Acad Med Singap., 38 (2009) 1004-6.
104. Moriyama K. Effect of temporary spinal cord stimulation on postherpetic neuralgia in the thoracic nerve area. Neuromodulation, 12 (2009) 39-43
105. Texakalidis P. et al. Neurosurgeons' Armamentarium for the Management of Refractory Postherpetic Neuralgia: A Systematic Literature Review. Stereotact Funct Neurosurg., 97 (2019) 55-65
106. Huang M. et al. Treatment Efficacy and Technical Advantages of Temporary Spinal Nerve Root Stimulation Compared to Traditional Spinal Cord Stimulation for Postherpetic Neuralgia. Pain Physician, 25 (2022) E863-E873
107. Larson S.J., Sances A., Riegel D.H., Meyer G.A., Dallmann D.E. and Swiontek T. Neurophysilogical effects of dorsal column stimulation in man and monkey. J.Neurosurg., 41 (1974) 217-223
108. Larson S.J., Sances A., Cusick J., Meyer G.A. and Swiontek T. A comparison between anterior and posterior spinal implant systems. Surg.Neurol., 4 (1975) 180-186
109. Hoppenstein R. Electrical stimulation of the ventral and dorsal column of the spinal cord for relief of chronic intractable pain: preliminary report. Surg.Neurol., 4 (1975a) 187-194
110. Hoppenstein R. Percutaneous implantation of chronic spinal cord electrodes for contro of intractable pain: preliminary report. Surg.Neurol., 4 (1975b) 195-198
111. Campbell J.N. and Taub A. Local analgesia from percutaneous electrical stimulation. A peripheral mechanism. Arch.Neurol., 28 (1973) 347-350
112. Ignelzi R.J. and Nyquist J.V. Direct effect of electrical stimulation on peripheral nerve evoked activity: implication in pain relief. J.Neurosurg., 45 (1976) 159-165
113. Adelman W.F., Fitzhugh R. Solution of the Hodgkin-Huxley equations modified for potassium accumulation in a periaxonal space. Fed.Proc., 34 (1975) 1322-1329
114. Campbell J.N. Examination of possible mechanisms by which stimulation of the spinal cord in man relieves pain. Appl.Neurophysiol., 44 (1980) 181-186
115. Friedman A.H., Nashold B.S. and Ovelmen‑Levitt J. Dorsal root entry zone lesions for the treatment of post‑herpetic neuralgia. J.Neurosurgery, 60 (1984) 1258‑1262
116. Nashold B.S. and Ostdahl R.H. Dorsal root entry zone lesions for pain relief. J.Neurosurg., 51 (1979) 59-69
117. Nashold B.S. and Ostdahl R.H. Pain relief after dorsal root entry zone lesions. Acta Neurochirurgica, Suppl.30 (1980) 383-389
118. Pagni C.A. e DeBenedittis G. La DREZ lesion: presupposti teorici, tecnica, indicazioni e risultati clinici. Atti IX Congresso Nazionale AISD, Sorrento 2-4 maggio 1986, Monduzzi Editore, Bologna 1987, pp.39-51
119. Nashold B.S.Jr. Current status of the DREZ operation. Neurosurgery, 15 (1984) 942-944
120. Melzack R. and Loeser J.D. Phantom body pain in paraplegics: evidence for a central 'pattern generating mechanism' for pain. Pain, 4 (1978) 195‑210
121. Loeser J.D. Definition, etiology and neurological assessment of pain originating in the nervous system following deafferentation. In Bonica J.J. et Al. (Eds.). Advances in pain research and therapy. Vol.5. Raven Press, New York 1983, pp.701-711
122. Yokota T. Neural mechanisms of trigeminal pain. In Fields H.L. et al. (Eds.). Advances in pain research and therapy. Vol.9. Raven Press, New York 1985, pp. 211-232
123. Hitchcock E.R. and Schvarcz J.R. Stereotaxic trigeminal tractotomy for post-herpetic facial pain. J.Neurosurg., 37 (1972) 412-417
124 Schvarcz J.R. Postherpetic craniofacial dysaesthesiae. Their management by stereotactic trigeminal nucleotomy. Acta Neurochir, 38 (1977) 65-72
125. Orlandini G. A new approach to spinal trigeminal nucleus: the lateral technique. In European Federation of IASP Chapters: Pain in Europe (1995). Abstract Book, p. 43
126. Yiping S., Jiayi S., Guang H., Yun J., Bingjie M., Xuehua H., Zhiyuan Y., Pingchuan M., Ke M. The efficacy and safety of epidural morphine/hydromorphone in the treatment of intractable postherpetic neuralgia: A single-center, double-blinded, randomized controlled, prospective, and non-inferiority study. Front Pharmacol., 13 (2022)
127. Mitas J.A. 2nd, Mosley C.A. Jr, Drager A.M. Diabetic neuropathic pain: control by amitriptyline and fluphenazine in renal insufficiency. South Med J., 76 (1983) 462-463
128. Raft D., Toomey T., Gregg J.M. Behavior modification and haloperidol in chronic facial pain. South Med J., 72 (1979) 155-159
129. Shir Y, Shenkman Z., Kaplan L. Neuropathic pain unrelieved by morphine, alleviated by haloperidol. Harefuah., 118 (1990) 452-454
130. McIver B,, Walsh D., Nelson K. The use of chlorpromazine for symptom control in dying cancer patients. J Pain Symptom Manage. 9 (1994) 341-345
131. Mehl-Madrona LE. Comparison of ketorolac-chlorpromazine with meperidine-promethazine for treatment of exacerbations of chronic pain. J Am B Fam Pract 1999; 12:188-194.
132. Lee SJ, Kim DH, Hahn SJ, Waxman SG, Choi JS. Mechanism of inhibition by chlorpromazine of the human pain threshold sodium channel, Nav1.7. Neurosci Lett., 639 (2017) 1-7.