Mindfulness as adjuvant therapy for chronic pain
Mindfulness come terapia adiuvante in pazienti affetti da dolore cronico
Clinical report
Pathos 2019, 26; 1. Online 2019, Apr 26
_______________________________________________________
Matteo L.G. Leoni1, Laura Bardetti2, Roberta Venturi1
and Fabrizio Micheli1
1Interventional Pain Unit, G. da Saliceto Hospital, Piacenza, Italy
2Clinical Psychologist
Summary
Mindfulness is a psychological treatment frequently used for the management of psychological distress, depressive symptoms and anxiety. It seems to work by refocusing the mind on the present with an increased awareness of inner sensations. Early mindfulness studies in chronic pain patients showed promising outcomes on pain and psychological symptoms even if the scientific evidence is poor due to methodological problems. The aim of this study was to find which chronic pain patients attending a self-help group would have chosen to practice mindfulness if they were asked and if there were prior individual features that made a patient best suited to this treatment. Our results suggest that only patients characterized by low levels of anxiety, depression and discomfort and high levels of wellness at CBA-VE score (Cognitive Behavioral Assessment) accepted to practice mindfulness. CBA-VE was able to differentiate between patients that accepted to practice mindfulness and who did not.
Riassunto
La mindfulness è un trattamento frequentemente utilizzato per la gestione del disagio psicologico, dei sintomi depressivi e dell'ansia; il trattamento consiste nel focalizzare la mente sul presente e nello sviluppare una maggiore consapevolezza sulle sensazioni interiori. Studi iniziali in pazienti con dolore cronico hanno mostrato risultati promettenti della mindfulness sul dolore e sui sintomi psicologici. Tuttavia alcuni problemi metodologici rendono limitata la loro evidenza scientifica. Lo scopo di questo studio è stato quello di conoscere quali pazienti con dolore cronico che frequentano un gruppo di auto–mutuo aiuto, avrebbero scelto di praticare la mindfulness se fosse stato loro richiesto, e quello di individuare delle caratteristiche individuali preliminari che avrebbero reso un paziente più adatto a questo trattamento. I nostri risultati suggeriscono che solo i pazienti caratterizzati da bassi livelli di ansia, depressione e disagio e alti livelli di benessere ottenuti al test CBA-VE (Cognitive Behavioral Assessment) accettano più facilmente di praticare la mindfulness. Il test CBA-VE è stato in grado di differenziare quali pazienti hanno accettato di praticare la mindfulness e quali non hanno mostrato alcun interesse.
Key words
mindfulness, chronic pain, psychological profile, self-help group
Parole chiave
mindfulness, dolore cronico, profilo psicologico, gruppo di auto-mutuo aiuto
Introduction
Mindfulness is the English equivalent of the ancient Pali words sati and sampajana, which can be translated as awareness, attention, insight and memory. Mindfulness is the human ability to be aware of where we are and what we are doing.1 It is the skill to non-judgmentally observe emotions, sensations, or cognition. Moreover it is a state of moment-to-moment awareness of thoughts, feelings, bodily sensations, and surrounding environment that is trained through meditation exercises.2,3 We can describe mindfulness as mindful awareness (awareness of awareness) and as mindful practice, (exercise base of acceptance commitment therapy).4 Mindfulness-based stress reduction (MBSR) is a treatment for psychological distress, depressive symptoms and anxiety that was developed by Kabat-Zinn for people with chronic disease.5
Chronic pain is a common disabling illness often related to high degrees of depressive symptoms6 and several psychological treatments have been suggested. Over the last few years a growing body of research has demonstrated that mindfulness-based interventions are associated with an enhancement of psychological well-being.7 The aim of our study was to find out which patients suffering from chronic pain would have chosen to practice mindfulness as adjuvant therapy and if there were prior individual features that made a patient best suited to this treatment.
Methods
Nineteen chronic pain patients without any prior meditative experience attending a psychological self-help group were asked to practice mindfulness as adjuvant therapy and were included in the present study. The self-help group is a group where people gather together, they tell their stories, share their experiences and their diseases in order to provide support for each other and to try to overcome their problems. Our self-help patients group is composed by some outpatients of our pain unit that, in a completely voluntary way, accepted to adhere to this kind of support. This group is supported by a non-profit association, open to all chronic pain patients, with the aim to give psychological support and to improve self-efficacy for managing pain.
All the enrolled patients provided written informed consent. The study was conducted at the Interventional Pain Unit of G. da Saliceto Hospital, Piacenza, Italy. Patients were given the opportunity of freely deciding whether they wanted to practice mindfulness or not. Consequently, two patients groups were spontaneously formed: MG (mindfulness group) and NMG (non-mindfulness group). The MG course was taught by a certified clinical psychologist who had completed specialized courses and training in mindfulness treatments. Mindfulness protocol was based on Mindfulness-based stress reduction (MBSR) revisited by Ronald D. Siegel.8 The program consisted of 9 week sessions (formal practice) with a duration of 1hour and 30 minutes each and homework practice for 20 minutes a day for 7 days a week. The main components of the program were meditation, hatha yoga and body scan (a sustained mindfulness practice in which attention is sequentially focused on different parts of the body).
In order to evaluate the clinical, psychological characteristics and results of the treatment, the following standardized tests have been selected: MAAS (Mindfulness Attention Awareness Scale), CBA-VE (Cognitive Behavioral Assessment), FFMQ (Five Facet Mindfulness Questionnaire), NRS (Numerical Rating Scale) and SF-12 (Short Form Health Survey). These tests were submitted at baseline (T0) and at the end of the mindfulness treatment (T1). Psychiatric co-morbidity, substance abuse, major psychiatric disorder that would prevent compliance, severe chronic medical conditions and inability to understand the protocol or the tests were considered as exclusion criteria. Demographic data, baseline questionnaires and clinical information were collected at enrollment. Continuous variables were analyzed using parametric statistic after normality distribution confirmation. Results are reported as mean±standard deviation, categorical variables are described by numbers and relative frequency (%). Statistical analysis was performed using SPSS v.25.0. Significance level was set at p< 0.05.
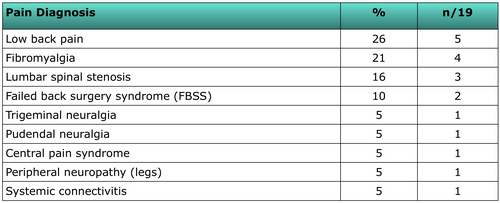
Nineteen patients with a median age of 63±13.5 years were enrolled. They were mainly females (79%). The sample was characterized by a great variability in pain diagnosis with low back pain and fibromyalgia as the most represented categories (Table 1).
{kind=link}
Results
Only ten patients accepted to practice mindfulness and to follow the study protocol, otherwise nine patients did not show any interest in this treatment. At baseline, a clear difference was found in CBA-VE score results between MG and NMG patients. In fact, anxiety (MG 17.6±4.22, NMG 34.2±1104, p 0.0006), wellness (MG 21±5.72, NMG 11.8±4.92, p 0.0021), perception (MG 19.2±4.76, NMG 13±3.97, p 0.0083), depression (MG 23.4±5.79, NMG 43.6±14.62, p 0.0015) and discomfort (MG 16.1±4.8, NMG 28.6±14.48, p 0.0263) were significantly worse in NMG compared to MG patients (Tab.2). Moreover NMG patients reported significantly higher pain level (NRS: 7.87±1.13) compared to MG (NRS: 6.11±1.45, p 0.01). No difference was found at T0 for MAAS (p=0.44), SF-12 (PCS-12 p 0.58; MCS-12 p=0.20), EQ-5D (p=0.99) and FFMQ subcategories, with the exclusion of observing/noticing parameter (p=0.014), (Table 2).
{kind=link}
A slightly increase in CBA-VE parameters, even if not statistically significant, was noticed in MG at the end of mindfulness treatment protocol (Anxiety: 17.6±4.22 (T0), 19.6±4.89 (T1), p=0.32; Wellness: 21±5.72 (T0) 19.6±4.57 (T1) p=0.29; Perception: 19.2±4.76 (T0), 20.4±3.05 (T1), p=0.52; Depression: 23.4±5.79 (T0), 26.2±6.79 (T1) p=0.37; Discomfort 16.1±4.8 (T0), 21.3±8.64 (T1), p=0.22). Moreover, in MG no difference was found in MAAS (p=0.72), SF-12 (PCS-12 p0.87, MCS-12 p=0.63), EQ-5D (p=0.82) and FFMQ subcategories at T1. NRS levels did not change after mindfulness (6.11±1.45 (T0), 6±1.12 (T1), p=0.84). In NMG, no difference was found at T1 compared to T0 in all the tests. Thirty per cent of patients reported an increase in NRS immediately at the end of mindfulness treatment.
One patient in MG experienced a self-limited adverse event reported as a temporary strong feeling of anger toward his pain condition and acute increase in perceived anxiety.
Half of the patients in MG reported some difficulties in mindfulness homework practice due to a lack of personal perseverance and confidence in the learned technique.
Discussion
Early mindfulness studies and reviews in chronic pain patients showed promising outcomes of this technique on pain and psychological symptoms.9-11 Mindfulness meditation seems to work by refocusing the mind on the present with an increased awareness of inner sensations. Unfortunately the lack of randomization, small sample size and some methodological problems should be considered as great limitation of these studies.
Our data suggests that only few chronic pain patients accepted to practice mindfulness if they were asked. In fact, only patients characterized by low levels of anxiety, depression and discomfort and higher levels of wellness and perception showed some interest in following our mindfulness program. CBA-VE test was able to differentiate between MG and NMG at T0. No difference was found in MAAS, SF-12, EQ-5D and FFMQ between MG and NMG. Only a slightly increase in CBA-VE parameters, even if not statistically significant, was observed at T1 in MG. No significant global clinical benefit was achieved with mindfulness in MG after the treatment. Accordingly to a recently published meta-analysis,12 mindfulness was associated only with a very small effect in improving pain symptoms. Our preliminary data suggest the existence of a subgroup of chronic pain patients more suitable to practice mindfulness. It is therefore of prominent importance to address mindfulness treatment to a selected and appropriate population if we want to test its effectiveness. CBA-VE test seems to uncover this subpopulation but these findings should be verified in a larger population.
Rosenzweig et al, reported a correlation between home mindfulness practice and a greater reduction in psychological distress and somatization symptoms.3 A half of our MG patients reported some difficulties in mindfulness homework practice due to a lack of personal perseverance and confidence in the learned technique. For this reason we can suppose that our results were underrated. Moreover, the poor findings of our study in terms of adverse events and lack of efficacy could also be related to the high prevalence of low back pain and fibromyalgia in the enrolled population. In fact, these patients are notably poor responsive to mindfulness treatments.12,13
The total length of mindfulness intervention program of our protocol is in line with previously published literature14 and no relations were found between program duration and clinical effect.12
This study presents several limitations. The first one is the small sample size that is related to limited number of our pain patients that accepted a psychological support and decided to participate to a self-help group. Another important limit is the lack of disability and depression evaluation with the use, for example, of some validated scales: Beck Depression Inventory, Patient Health Questionnaire, Roland-Morris Disability Questionnaire, Sheehan Disability Scale. Therefore it is difficult to understand if mindfulness provided a specific clinical benefit not in pain reduction but in disability improvement. No long term follow-up was planned and no data on analgesic use were collected. Another important limit is the absence of any randomization that reduces the relevance of the present study that is only observational.
Conclusions
Our preliminary data suggest the existence of a subgroup of chronic pain patients more suitable to practice mindfulness. It is therefore of prominent importance to address mindfulness treatment to a selected and appropriate population if we want to test its effectiveness. CBA-VE test seems to uncover this subpopulation but these findings should be verified in a larger population. Unfortunately the clinical benefit of mindfulness in chronic pain patients is still lacking. More studies are needed to better understand whether mindfulness treatments directed to correct patients can have a role as adjuvant therapy to manage chronic pain.
Conflict of interests
The authors certify the study was conducted without conflicts of interests.
Published
30th March 2019
References
1) Brown KW, Ryan RM. The Benefits of Being Present: Mindfulness and Its Role in Psychological Well-Being. Journal of Personality and Social Psychology 2003; 84, 822-848.
2) Kabat-Zinn J. Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness (1990). New York, NY Pub by Dell Publishing, a division of Bantam Doubleday Dell Pub Group, 1991.